Department of Gastroenterology, University Hospital CHU of Liège, Liège, Belgium.
Université de Paris, ECSTRRA - CRESS UMR1153, INSERM and SBIM, AP-HP, Hôpital Saint-Louis, Paris, France.
Lancet Gastroenterol Hepatol. 2023 Mar;8(3):215-227. doi: 10.1016/S2468-1253(22)00385-5. Epub 2023 Jan 11.
The combination of infliximab and immunosuppressant therapy is a standard management strategy for patients with Crohn's disease. Concerns regarding the implications of long-term combination therapy provided the rationale for a formal clinical trial of treatment de-escalation. Our aim was to compare the relapse rate and the time spent in remission over 2 years between patients continuing combination therapy and those stopping infliximab or immunosuppressant therapy.
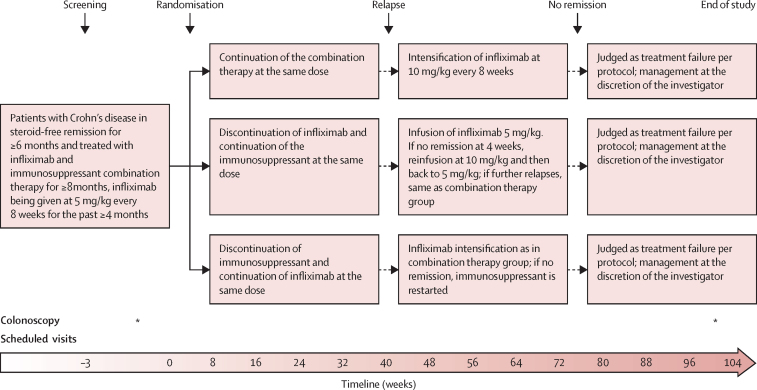
This multicentre, open-label, randomised controlled trial was performed in 64 hospitals in seven countries in Europe and Australia. Adult patients with Crohn's disease in steroid-free clinical remission for more than 6 months, on combination therapy of infliximab and immunosuppressant therapy for at least 8 months were randomly assigned (1:1:1) to either continue combination therapy (combination group), discontinue infliximab (infliximab withdrawal group), or discontinue immunosuppressant therapy (immunosuppressant withdrawal group). Randomisation was stratified according to disease duration before start of first anti-TNF treatment (≤2 or >2 years), failure of immunosuppressant therapy before start of infliximab, and presence of ulcers at baseline endoscopy. The patient number and group of each stratum were assigned by a central online randomisation website. Treatment was optimised or resumed in case of relapse in all groups. Participants, those assessing outcomes, and those analysing the data were not masked to group assignment. The coprimary endpoints were the relapse rate (superiority analysis) and time in remission over 2 years (non-inferiority analysis, non-inferiority margin 35 days). Analyses were done on an intention-to-treat basis. This study is registered with ClinicalTrials.gov, NCT02177071, and with EU Clinical Trials Register, EUDRACT 2014-002311-41. The trial was completed in April, 2021.
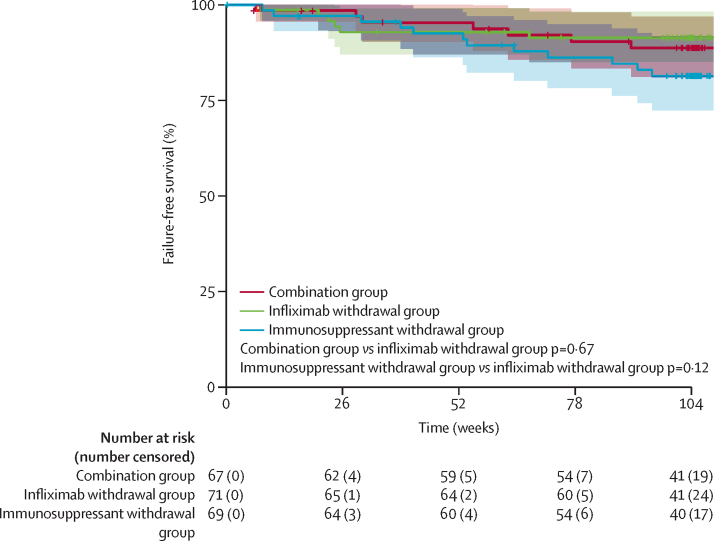
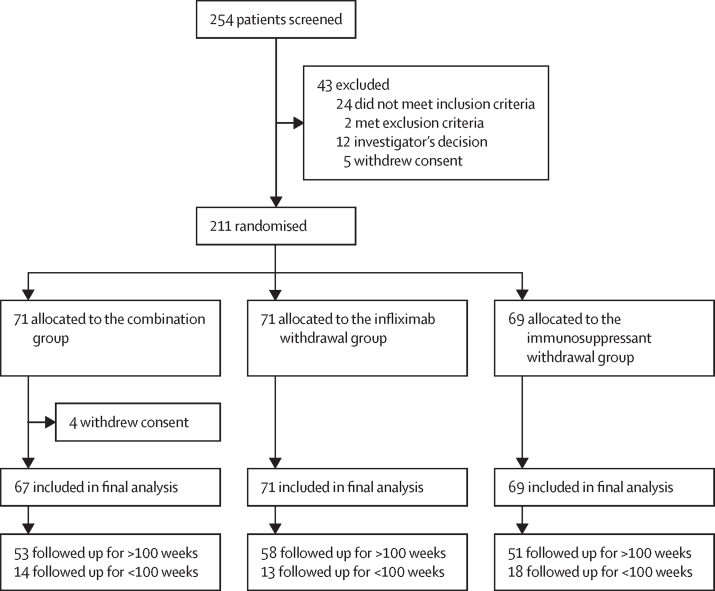
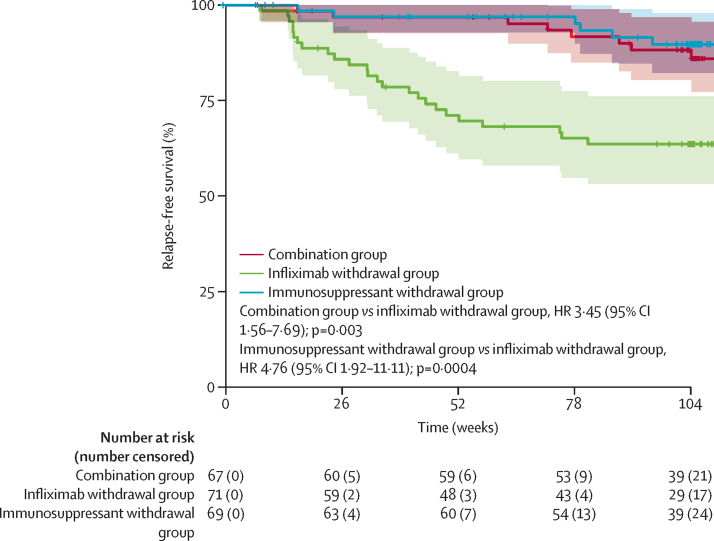
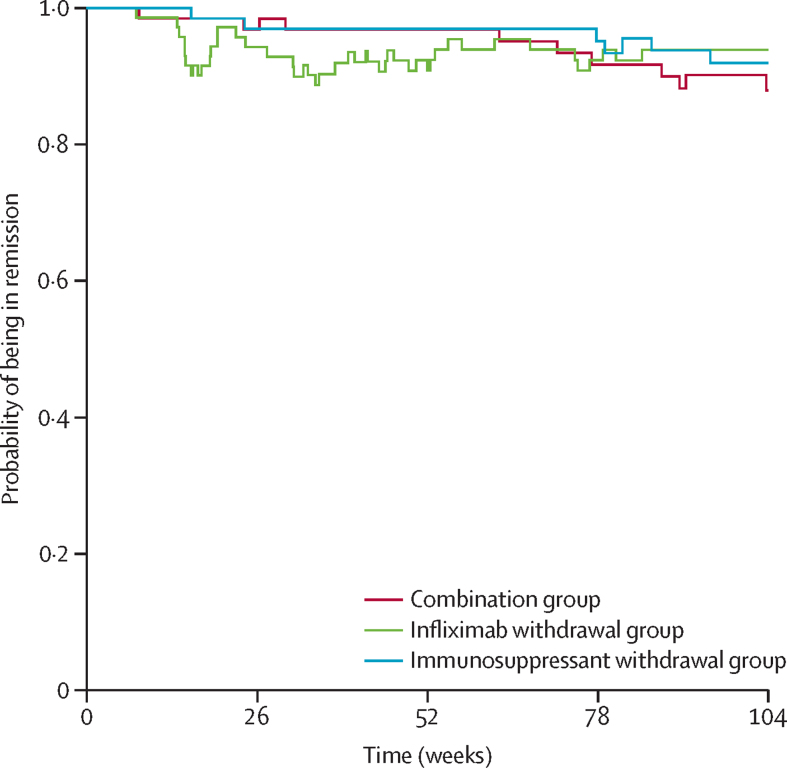
Between Nov 2, 2015, and April 24, 2019, 254 patients were screened. Of these, 211 were randomised and 207 were included in the final analysis (n=67 in the combination group, n=71 in the infliximab withdrawal group, and n=69 in the immunosuppressant withdrawal group). 39 patients had a relapse (eight [12%] of 67 in the combination group, 25 [35%] of 71 in the infliximab withdrawal group, six [9%] of 69 in the immunosuppressant withdrawal group). 2-year relapse rates were 14% (95% CI 4-23) in the combination group, 36% (24-47) in the infliximab withdrawal group, and 10% (2-18) in the immunosuppressant withdrawal group (hazard ratio [HR] 3·45 [95% CI 1·56-7·69], p=0·003, for infliximab withdrawal vs combination, and 4·76 [1·92-11·11], p=0·0004, for infliximab withdrawal vs immunosuppressant withdrawal). Of 28 patients who had a relapse and were retreated or optimised according to protocol, remission was achieved in 25 patients (one of two in the combination group, 22 of 23 in the infliximab withdrawal group, and two of three in the immunosuppressant withdrawal group). The mean time spent in remission over 2 years was 698 days (95% CI 668-727) in the combination group, 684 days (651-717) in the infliximab withdrawal group, and 706 days (682-730) in the immunosuppressant withdrawal group. The difference in restricted mean survival time in remission was -14 days (95% CI -56 to 27) between the infliximab withdrawal group and the combination group and -22 days (-62 to 16) between the infliximab withdrawal group and the immunosuppressant withdrawal group. The 95% CIs contained the non-inferiority threshold (-35 days). We recorded 31 serious adverse events, in 20 patients, with no difference in frequency between groups. The most frequent serious adverse events were infections (four in the combination group, two in the infliximab withdrawal group, and one in the immunosuppressant withdrawal group) and Crohn's disease exacerbation (three in the combination group, four in the infliximab withdrawal group, and one in the immunosuppressant withdrawal group). No death nor malignancy was recorded.
In patients with Crohn's disease in sustained steroid-free remission under combination therapy with infliximab and immunosuppressant therapy, withdrawal of infliximab should only be considered after careful assessment of risks and benefits for each patient, whereas withdrawal of immunosuppressant therapy could generally represent a preferable strategy when considering treatment de-escalation.
European Union's Horizon 2020.
英夫利昔单抗联合免疫抑制剂治疗是克罗恩病患者的标准治疗方案。对长期联合治疗的影响的担忧为正式的治疗降级临床试验提供了依据。我们的目的是比较继续联合治疗组与停止英夫利昔单抗或免疫抑制剂治疗组的 2 年内复发率和缓解时间。
本研究为多中心、开放标签、随机对照试验,在欧洲和澳大利亚的 7 个国家的 64 家医院进行。无激素治疗且缓解时间超过 6 个月、至少接受过 8 个月英夫利昔单抗联合免疫抑制剂治疗的成人克罗恩病患者,按 1:1:1 比例随机分为继续联合治疗组(联合组)、停止英夫利昔单抗组(英夫利昔单抗停药组)或停止免疫抑制剂组(免疫抑制剂停药组)。随机分组按开始抗 TNF 治疗前的疾病持续时间(≤2 年或>2 年)、开始英夫利昔单抗治疗前免疫抑制剂治疗失败情况以及基线内镜下溃疡存在情况进行分层。通过中央在线随机网站分配每个分层的患者数量和组。所有组在复发时均优化或恢复治疗。参与者、评估结果的人员和分析数据的人员对分组情况不知情。主要终点为复发率(优效性分析)和 2 年内缓解时间(非劣效性分析,非劣效性边界 35 天)。采用意向治疗进行分析。本研究在 ClinicalTrials.gov 注册,NCT02177071,并在欧盟临床试验注册处,EUDRACT 2014-002311-41 注册。试验于 2021 年 4 月完成。
2015 年 11 月 2 日至 2019 年 4 月 24 日,共筛选了 254 名患者。其中,211 名患者被随机分组,207 名患者纳入最终分析(联合组 67 例,英夫利昔单抗停药组 71 例,免疫抑制剂停药组 69 例)。39 名患者出现复发(联合组 8 例[12%],英夫利昔单抗停药组 25 例[35%],免疫抑制剂停药组 6 例[9%])。2 年复发率分别为联合组 14%(95%CI 4-23)、英夫利昔单抗停药组 36%(24-47)和免疫抑制剂停药组 10%(2-18)(英夫利昔单抗停药组 vs 联合组 HR 3.45[95%CI 1.56-7.69],p=0.003,英夫利昔单抗停药组 vs 免疫抑制剂停药组 HR 4.76[1.92-11.11],p=0.0004)。28 名复发并根据方案进行再治疗或优化的患者中,25 名患者缓解(联合组 2 名中的 1 名,英夫利昔单抗停药组 23 名中的 22 名,免疫抑制剂停药组 3 名中的 2 名)。2 年内缓解时间分别为联合组 698 天(95%CI 668-727)、英夫利昔单抗停药组 684 天(651-717)和免疫抑制剂停药组 706 天(682-730)。英夫利昔单抗停药组与联合组间的限制性平均生存时间差异为-14 天(95%CI -56 至 27),英夫利昔单抗停药组与免疫抑制剂停药组间的差异为-22 天(95%CI -62 至 16)。95%CI 包含非劣效性边界(-35 天)。我们记录了 31 例严重不良事件,涉及 20 名患者,各组之间无差异。最常见的严重不良事件是感染(联合组 4 例,英夫利昔单抗停药组 2 例,免疫抑制剂停药组 1 例)和克罗恩病加重(联合组 3 例,英夫利昔单抗停药组 4 例,免疫抑制剂停药组 1 例)。无死亡或恶性肿瘤病例。
在接受英夫利昔单抗联合免疫抑制剂治疗并处于持续无激素缓解的克罗恩病患者中,只有在仔细评估每位患者的风险和获益后,才应考虑停止英夫利昔单抗治疗,而停止免疫抑制剂治疗通常可以作为考虑治疗降级的更优策略。
欧盟地平线 2020 计划。