Department of Medicine.
Wellcome Centre for Infectious Diseases Research in Africa, Institute of Infectious Disease and Molecular Medicine.
Clin Infect Dis. 2023 May 24;76(10):1832-1840. doi: 10.1093/cid/ciad023.
Dolutegravir concentrations are reduced by efavirenz induction effect necessitating twice-daily dolutegravir dosing when coadministered. Efavirenz induction persists for several weeks after stopping, which could potentially select for dolutegravir resistance if switching occurred with unsuppressed human immunodeficiency virus type 1 (HIV-1) RNA levels and standard dolutegravir dosing. We evaluated the need for a lead-in supplementary dolutegravir dose in adults failing first-line tenofovir-emtricitabine-efavirenz (TEE).
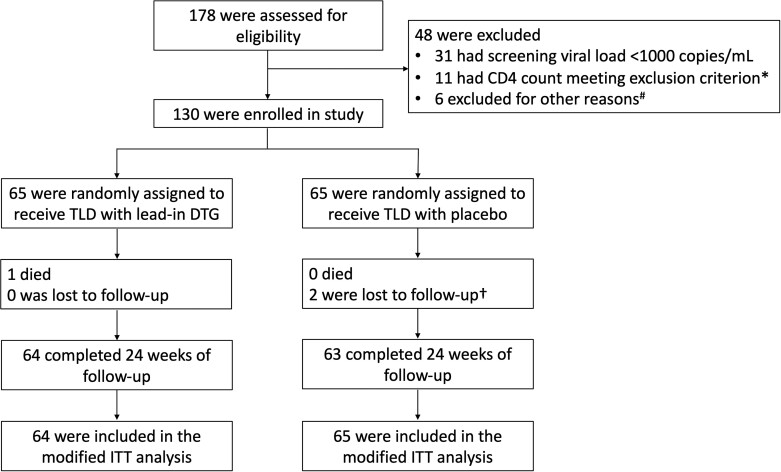
We conducted a randomized, double-blind, placebo-controlled, phase 2 trial in Khayelitsha, South Africa. Eligible patients had virologic failure (2 consecutive HIV-1 RNA ≥1000 copies/mL) on first-line TEE. Participants were randomly assigned (1:1) to switch to tenofovir-lamivudine-dolutegravir (TLD) with a supplementary 50 mg dolutegravir dose or placebo taken 12 hours later for 14 days. Primary outcome was proportion with HIV-1 RNA <50 copies/mL at week 24. This study was not powered to compare arms.
One hundred thirty participants were randomized (65 to each arm). Median baseline HIV-1 RNA was 4.0 log10 copies/mL and 76% had baseline resistance to both tenofovir and lamivudine. One participant died and 2 were lost to follow-up. At week 24, 55 of 64 (86% [95% confidence interval {CI}: 75%-93%]) in the supplementary dolutegravir arm and 53 of 65 (82% [95% CI: 70%-90%]) in the placebo arm had HIV-1 RNA <50 copies/mL. Grade 3 or 4 adverse events were similar in frequency between arms. None of 6 participants (3 in each arm) eligible for resistance testing by 24 weeks developed dolutegravir resistance.
Our findings do not support the need for initial dolutegravir dose adjustment in patients switching to TLD who failed first-line TEE.
NCT03991013.
当与依非韦伦共同给药时,依非韦伦的诱导作用会降低多替拉韦的浓度,因此需要每日两次给予多替拉韦。依非韦伦诱导作用在停药后持续数周,这可能会在人类免疫缺陷病毒 1 型(HIV-1)RNA 水平未得到抑制且标准多替拉韦剂量给药的情况下切换时选择多替拉韦耐药。我们评估了在最初使用替诺福韦-恩曲他滨-依非韦伦(TEE)治疗失败的成人中,是否需要先导补充多替拉韦剂量。
我们在南非开普敦进行了一项随机、双盲、安慰剂对照、2 期试验。符合条件的患者在最初使用 TEE 时出现病毒学失败(连续 2 次 HIV-1 RNA≥1000 拷贝/mL)。参与者被随机分配(1:1)至替诺福韦-拉米夫定-多替拉韦(TLD)组,同时给予补充 50mg 多替拉韦剂量或安慰剂,12 小时后服用 14 天。主要结局是第 24 周时 HIV-1 RNA<50 拷贝/mL 的比例。该研究没有足够的能力来比较两组。
130 名参与者被随机分配(每组 65 名)。中位基线 HIV-1 RNA 为 4.0 log10 拷贝/mL,76%的患者对替诺福韦和拉米夫定均有基线耐药性。1 名参与者死亡,2 名参与者失访。第 24 周时,补充多替拉韦组有 64 名中的 55 名(86%[95%置信区间:75%-93%])和安慰剂组有 65 名中的 53 名(82%[95%置信区间:70%-90%])HIV-1 RNA<50 拷贝/mL。两组之间不良事件的 3 级或 4 级发生率相似。24 周时符合耐药性检测条件的 6 名参与者(每组 3 名)均未发现多替拉韦耐药。
我们的研究结果不支持在最初使用 TEE 治疗失败后改用 TLD 的患者中,初始多替拉韦剂量需要调整。
NCT03991013。