Division of Clinical Pharmacology, Department of Medicine, University of Cape Town, Cape Town, South Africa; Wellcome Centre for Infectious Diseases Research in Africa, Institute of Infectious Disease and Molecular Medicine, and Department of Medicine, University of Cape Town, Cape Town, South Africa.
Wellcome Centre for Infectious Diseases Research in Africa, Institute of Infectious Disease and Molecular Medicine, and Department of Medicine, University of Cape Town, Cape Town, South Africa; Department of Medicine, University of Cape Town, Cape Town, South Africa.
Lancet HIV. 2023 Jul;10(7):e433-e441. doi: 10.1016/S2352-3018(23)00081-4. Epub 2023 May 22.
The drug-drug interaction between rifampicin and dolutegravir can be overcome by supplemental dolutegravir dosing, which is difficult to implement in high-burden settings. We aimed to test whether virological outcomes with standard-dose dolutegravir-based antiretroviral therapy (ART) are acceptable in people with HIV on rifampicin-based antituberculosis therapy.
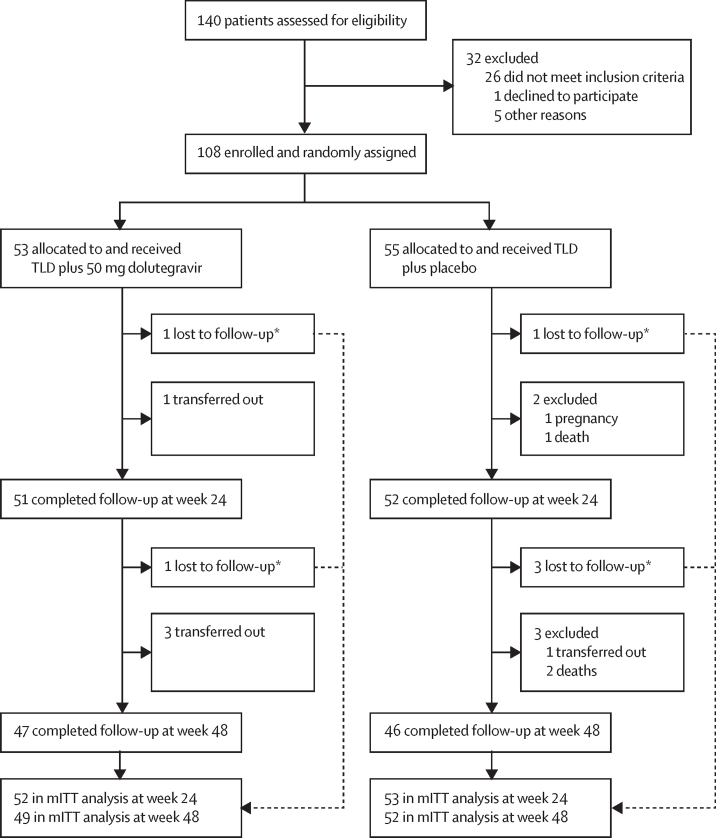
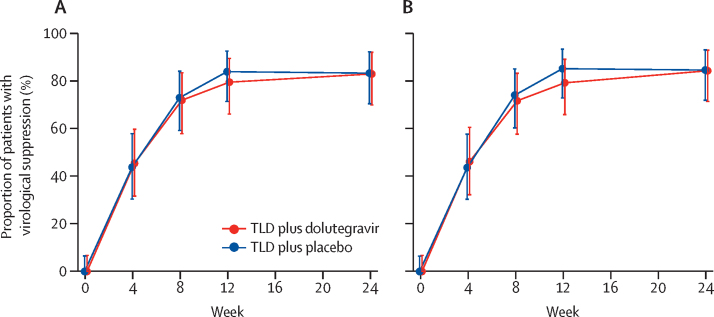
RADIANT-TB was a phase 2b, randomised, double-blind, non-comparative, placebo-controlled trial at a single site in Khayelitsha, Cape Town, South Africa. Participants were older than 18 years of age, with plasma HIV-1 RNA greater than 1000 copies per mL, CD4 count greater than 100 cells per μL, ART-naive or first-line ART interrupted, and on rifampicin-based antituberculosis therapy for less than 3 months. By use of permuted block (block size of 6) randomisation, participants were assigned (1:1) to receive either tenofovir disoproxil fumarate, lamivudine, and dolutegravir plus supplemental 50 mg dolutegravir 12 h later or tenofovir disoproxil fumarate, lamivudine, and dolutegravir plus matched placebo 12 h later. Participants received standard antituberculosis therapy (rifampicin, isoniazid, pyrazinamide, and ethambutol for the first 2 months followed by isoniazid and rifampicin for 4 months). The primary outcome was the proportion of participants with virological suppression (HIV-1 RNA <50 copies per mL) at week 24 analysed in the modified intention-to-treat population. This study is registered with ClinicalTrials.gov, NCT03851588.
Between Nov 28, 2019, and July 23, 2021, 108 participants (38 female, median age 35 years [IQR 31-40]) were randomly assigned to supplemental dolutegravir (n=53) or placebo (n=55). Median baseline CD4 count was 188 cells per μL (IQR 145-316) and median HIV-1 RNA was 5·2 log copies per mL (4·6-5·7). At week 24, 43 (83%, 95% CI 70-92) of 52 participants in the supplemental dolutegravir arm and 44 (83%, 95% CI 70-92) of 53 participants in the placebo arm had virological suppression. No treatment-emergent dolutegravir resistance mutations were detected up to week 48 in the 19 participants with study-defined virological failure. Grade 3 and 4 adverse events were similarly distributed between the study arms. The most frequent grade 3 and 4 adverse events were weight loss (4/108 [4%]), insomnia (3/108 [3%]), and pneumonia (3/108 [3%]).
Our findings suggest that twice-daily dolutegravir might be unnecessary in people with HIV-associated tuberculosis.
Wellcome Trust.
利福平与多替拉韦之间的药物相互作用可以通过补充多替拉韦剂量来克服,但在高负担环境中难以实施。我们旨在检验在接受利福平为基础的抗结核治疗的 HIV 感染者中,接受标准剂量多替拉韦为基础的抗逆转录病毒治疗(ART)的病毒学结果是否可以接受。
RADIANT-TB 是在南非开普敦 Khayelitsha 的一个单一地点进行的 2b 期、随机、双盲、非对照、安慰剂对照试验。参与者年龄大于 18 岁,血浆 HIV-1 RNA 大于 1000 拷贝/毫升,CD4 计数大于 100 个/μL,为初治或一线 ART 中断,且接受利福平为基础的抗结核治疗不到 3 个月。通过使用置换块(块大小为 6)随机化,参与者被随机分配(1:1)接受替诺福韦二吡呋酯、拉米夫定和多替拉韦,以及 12 小时后补充 50mg 多替拉韦,或替诺福韦二吡呋酯、拉米夫定和多替拉韦,以及 12 小时后补充匹配的安慰剂。参与者接受标准的抗结核治疗(前 2 个月使用利福平、异烟肼、吡嗪酰胺和乙胺丁醇,然后 4 个月使用异烟肼和利福平)。主要终点是在改良意向治疗人群中,在第 24 周时具有病毒学抑制(HIV-1 RNA<50 拷贝/毫升)的参与者比例。本研究在 ClinicalTrials.gov 注册,NCT03851588。
在 2019 年 11 月 28 日至 2021 年 7 月 23 日期间,108 名参与者(38 名女性,中位年龄 35 岁[IQR 31-40])被随机分配至补充多替拉韦(n=53)或安慰剂(n=55)组。中位基线 CD4 计数为 188 个/μL(IQR 145-316),中位 HIV-1 RNA 为 5.2 log 拷贝/毫升(4.6-5.7)。在第 24 周时,补充多替拉韦组的 52 名参与者中有 43 名(83%,95%CI 70-92)和安慰剂组的 53 名参与者中有 44 名(83%,95%CI 70-92)达到病毒学抑制。在 19 名具有研究定义的病毒学失败的参与者中,直至第 48 周,未检测到新发的多替拉韦耐药突变。研究组之间的 3 级和 4 级不良事件分布相似。最常见的 3 级和 4 级不良事件是体重减轻(4/108[4%])、失眠(3/108[3%])和肺炎(3/108[3%])。
我们的研究结果表明,在 HIV 相关结核病患者中,每日两次多替拉韦可能是不必要的。
威康信托基金会。