Hireche Kheira, Lounes Youcef, Bacri Christophe, Solovei Laurence, Marty-Ané Charles, Canaud Ludovic, Alric Pierre
Department of Thoracic and Vascular Surgery, Arnaud de Villeneuve University Hospital, 34090 Montpellier, France.
PhyMedExp, INSERM, CNRS, University of Montpellier, 34295 Montpellier, France.
Cancers (Basel). 2023 Jan 8;15(2):414. doi: 10.3390/cancers15020414.
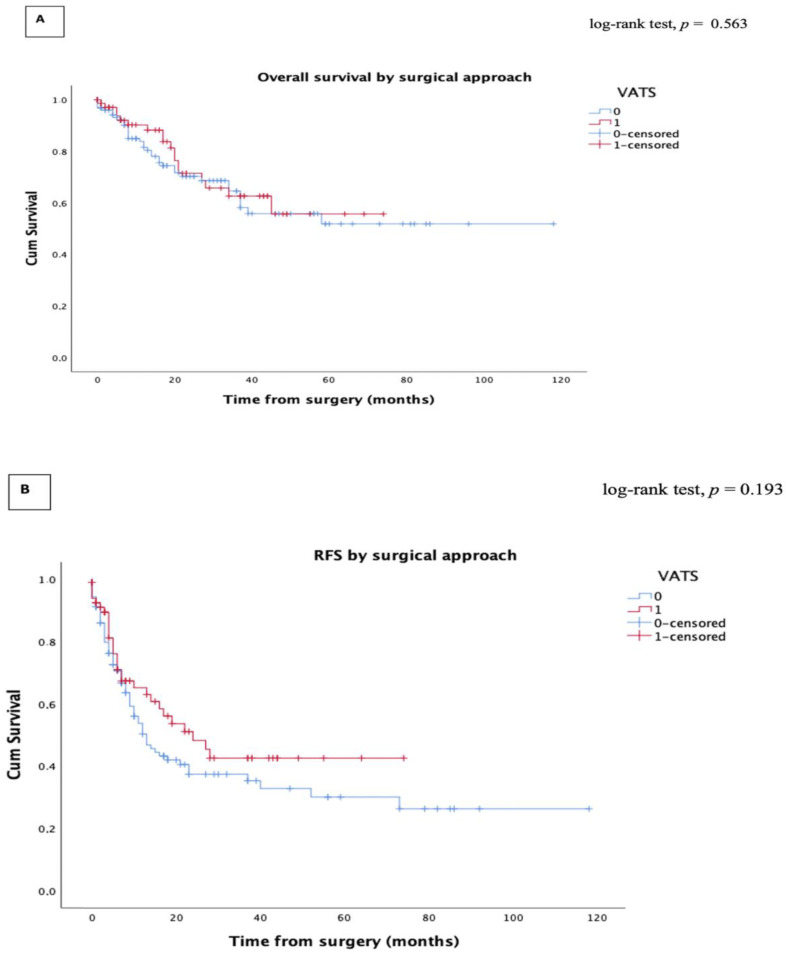
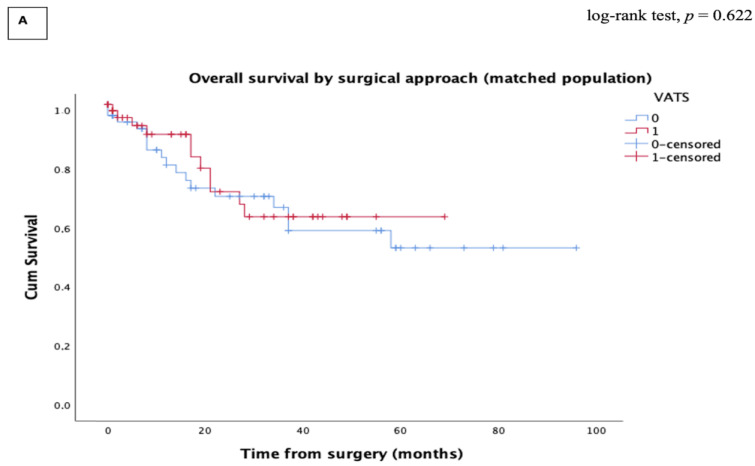
Objectives: This study aims to evaluate the perioperative and oncologic outcomes of thoracoscopic lobectomy for advanced stage III NSCLC. Methods: We retrospectively reviewed 205 consecutive patients who underwent VATS or open lobectomy for clinical stage III lung cancer between January 2013 and December 2020. The perioperative and oncologic outcomes of the two approaches were compared. Long-term survival was assessed using the Kaplan−Meier estimator. Propensity score-matched (PSM) comparisons were used to obtain a well-balanced cohort of patients undergoing VATS and open lobectomy. Results: VATS lobectomy was performed in 77 (37.6%) patients and open lobectomy in 128 (62.4%) patients. Twelve patients (15.6%) converted from VATS to the open approach. PSM resulted in 64 cases in each group, which were well matched according to twelve potential prognostic factors, including tumor size, histology, and pTNM stage. Between the VATS and the open group, there were no significant differences in unmatched and matched analyses, respectively, of the overall postoperative complications (p = 0.138 vs. p = 0.109), chest tube duration (p = 0.311 vs. p = 0.106), or 30-day mortality (p = 1 vs. p = 1). However, VATS was associated with shorter hospital stays (p < 0.0001). The five-year overall survival (OS) and five-year Recurrence-free survival (RFS) were comparable between the VATS and the open groups. There was no significant difference in the recurrence pattern between the two groups in both the unmatched and matched analyses. Conclusion: For the advanced stage III NSCLC, VATS lobectomy achieved equivalent postoperative and oncologic outcomes when compared with open lobectomy without increasing the risk of procedure-related locoregional recurrence.
本研究旨在评估晚期Ⅲ期非小细胞肺癌(NSCLC)胸腔镜肺叶切除术的围手术期和肿瘤学结局。方法:我们回顾性分析了2013年1月至2020年12月期间连续接受电视辅助胸腔镜手术(VATS)或开放性肺叶切除术治疗临床Ⅲ期肺癌的205例患者。比较了两种手术方式的围手术期和肿瘤学结局。采用Kaplan-Meier估计器评估长期生存率。使用倾向评分匹配(PSM)比较来获得接受VATS和开放性肺叶切除术的平衡良好的患者队列。结果:77例(37.6%)患者接受了VATS肺叶切除术,128例(62.4%)患者接受了开放性肺叶切除术。12例患者(15.6%)从VATS转为开放手术。PSM后每组有64例,根据包括肿瘤大小、组织学和pTNM分期在内的12个潜在预后因素进行了良好匹配。在VATS组和开放组之间,未匹配和匹配分析中总体术后并发症(p = 0.138对p = 0.109)、胸管留置时间(p = 0.311对p = 0.106)或30天死亡率(p = 1对p = 1)分别无显著差异。然而,VATS与较短的住院时间相关(p < 0.0001)。VATS组和开放组之间的五年总生存率(OS)和五年无复发生存率(RFS)相当。在未匹配和匹配分析中,两组之间的复发模式均无显著差异。结论:对于晚期Ⅲ期NSCLC,与开放性肺叶切除术相比,VATS肺叶切除术在不增加手术相关局部区域复发风险的情况下,实现了相当的术后和肿瘤学结局。