Corradi Francesco, Santori Gregorio, Brusasco Claudia, Robba Chiara, Wong Adrian, Di Nicolò Pierpaolo, Tecchi Ludovica, Dazzi Federico, Taddei Erika, Isirdi Alessandro, Coccolini Federico, Forfori Francesco, Tavazzi Guido
Department of Surgical, Medical, Molecular Pathology and Critical Care Medicine, University of Pisa, 56126 Pisa, Italy.
Azienda Ospedaliero Universitaria Pisana, Via Paradisa, 2, 56124 Pisa, Italy.
J Clin Med. 2023 Jan 16;12(2):700. doi: 10.3390/jcm12020700.
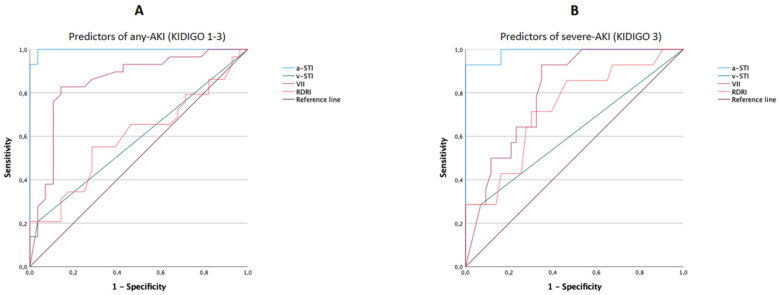
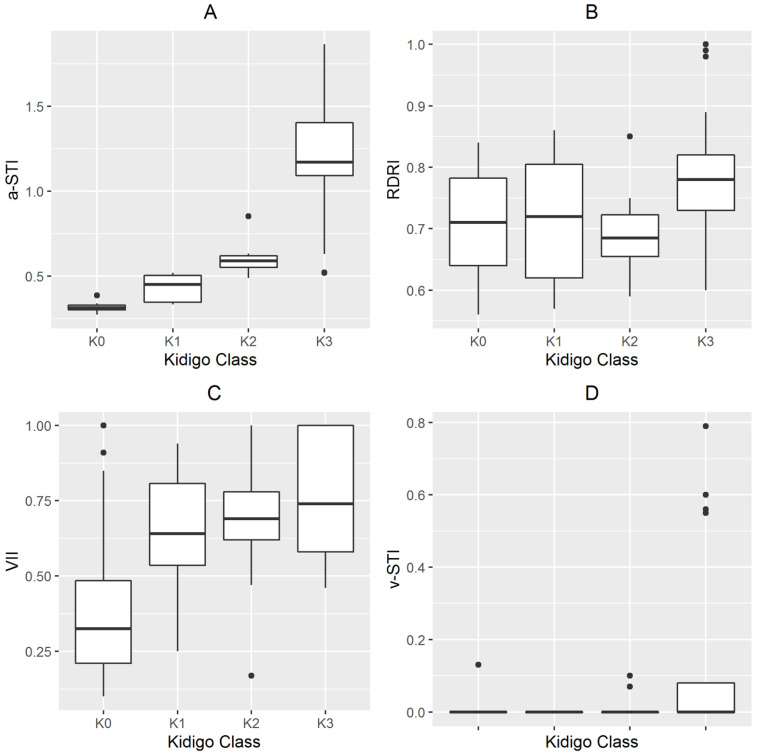
Background: Acute kidney injury (AKI) is common in critically ill patients admitted to intensive care units (ICU) and is frequently associated with poorer outcomes. Hence, if an indicator is available for predicting severe AKI within the first few hours of admission, management strategies can be put into place to improve outcomes. Materials and methods: This was a prospective, observational study, involving 63 critically ill patients, that aimed to explore the diagnostic accuracy of different Doppler parameters in predicting AKI in critically ill patients from a mixed ICU. Participants were enrolled at ICU admission. All underwent ultrasonographic examinations and hemodynamic assessment. Renal Doppler resistive index (RDRI), venous impedance index (VII), arterial systolic time intervals (a-STI), and venous systolic time intervals (v-STI) were measured within 2 h from ICU admission. Results: Cox proportional hazards models, including a-STI, v-STI, VII, and RDRI as independent variables, returned a-STI as the only putative predictor for the development of AKI or severe AKI. An overall statistically significant difference (p < 0.001) was observed in the Kaplan−Meier plots for cumulative AKI events between patients with a-STI higher or equal than 0.37 and for cumulative severe AKI-3 between patients with a-STI higher or equal than 0.63. As assessed by the area under the receiver operating curves (ROC) curves, a-STI performed best in diagnosing any AKI and/or severe AKI-3. Positive correlations were found between a-STI and the N-terminal brain natriuretic peptide precursor (NT-pro BNP) (ρ = 0.442, p < 0.001), the sequential organ failure assessment (SOFA) score (ρ: 0.361, p = 0.004), and baseline serum creatinine (ρ: 0.529, p < 0.001). Conclusions: Critically ill patients who developed AKI had statistically significant different a-STI (on admission to ICU), v-STI, and VII than those who did not. Moreover, a-STI was associated with the development of AKI at day 5 and provided the best diagnostic accuracy for the diagnosis of any AKI or severe AKI compared with RDRI, VII, and v-STI.
急性肾损伤(AKI)在入住重症监护病房(ICU)的重症患者中很常见,且常与较差的预后相关。因此,如果能有一个指标可在入院后的头几个小时内预测严重AKI,就可以制定管理策略来改善预后。材料与方法:这是一项前瞻性观察性研究,纳入了63例重症患者,旨在探讨不同多普勒参数对混合ICU中重症患者AKI的诊断准确性。参与者在ICU入院时登记入组。所有人均接受了超声检查和血流动力学评估。在入住ICU后2小时内测量肾多普勒阻力指数(RDRI)、静脉阻抗指数(VII)、动脉收缩时间间期(a-STI)和静脉收缩时间间期(v-STI)。结果:以a-STI、v-STI、VII和RDRI作为自变量的Cox比例风险模型显示,a-STI是AKI或严重AKI发生的唯一假定预测因子。在a-STI高于或等于0.37的患者与a-STI低于0.37的患者之间,累积AKI事件的Kaplan-Meier曲线存在总体统计学显著差异(p < 0.001);在a-STI高于或等于0.63的患者与a-STI低于0.63的患者之间,累积严重AKI-3的Kaplan-Meier曲线也存在总体统计学显著差异(p < 0.001)。通过受试者操作特征曲线(ROC)下面积评估,a-STI在诊断任何AKI和/或严重AKI-3方面表现最佳。a-STI与N末端脑钠肽前体(NT-pro BNP)(ρ = 0.442,p < 0.001)、序贯器官衰竭评估(SOFA)评分(ρ:0.361,p = 0.004)和基线血清肌酐(ρ:0.529,p < 0.001)之间存在正相关。结论:发生AKI的重症患者在(入住ICU时)的a-STI、v-STI和VII与未发生AKI的患者相比,在统计学上有显著差异。此外,a-STI与第5天AKI的发生相关,并且与RDRI、VII和v-STI相比,在诊断任何AKI或严重AKI方面具有最佳的诊断准确性。