Hashemi Djawid, Doeblin Patrick, Blum Moritz, Weiss Karl Jakob, Schneider Matthias, Korosoglou Grigorios, Beyer Rebecca Elisabeth, Pieske Burkert, Edelmann Frank, Kelle Sebastian
Department of Internal Medicine and Cardiology, Charité - Universitätsmedizin Berlin, Charité Campus Virchow Clinic, Berlin, Germany.
Department of Internal Medicine and Cardiology, German Heart Institute Berlin (DHZB), Berlin, Germany.
Front Cardiovasc Med. 2023 Jan 5;9:1091768. doi: 10.3389/fcvm.2022.1091768. eCollection 2022.
The main management strategy of heart failure with preserved ejection fraction (HFpEF) is prevention since HFpEF is associated with many cardiovascular (CV) risk factors, especially since HFpEF is linked to a high risk for both mortality and recurrent heart failure (HF) hospitalizations. Therefore, there is a need for new tools to identify patients with a high risk profile early. Regional strain assessment by CMR seems to be superior in describing deformation impairment in HF. The MyoHealth score is a promising tool to identify cardiac changes early.
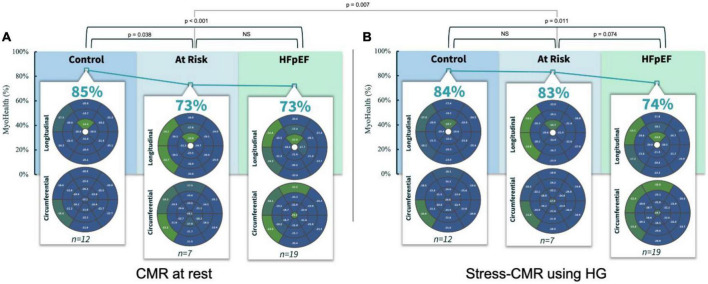
Heart failure patients irrespective of LVEF and asymptomatic controls were recruited, and CMR based measures were obtained. For this analysis the asymptomatic control group ( = 19) was divided into asymptomatic subjects without CV co-morbidities or evidence of cardiac abnormalities and ( = 12) and asymptomatic subjects with CV co-morbidities or evidence of cardiac abnormalities ( = 7) as well as patients with HFpEF ( = 19). We performed CMR scans at rest and during a stress test using isometric handgrip exercise (HG). Assessing the MyoHealth score at rest revealed preserved regional strain in 85 ± 9% of LV segments in controls, 73 ± 11% in at Risk subjects and 73 ± 8% in HFpEF patients. During stress the MyoHealth score was 84 ± 7% in controls, 83 ± 7 in at risk subjects and 74 ± 11 in HFpEF patients.
In summary, we show for the first time that asymptomatic subjects with increased CV risk present with HFpEF like impaired myocardial deformation at rest, while they show results like controls under HG stress. The potential of preventive treatment in this group of patients merits further investigation in future.
[https://drks.de/search/de/trial/DRKS00015615], identifier [DRKS00015615].
射血分数保留的心力衰竭(HFpEF)的主要管理策略是预防,因为HFpEF与许多心血管(CV)危险因素相关,特别是因为HFpEF与死亡和复发性心力衰竭(HF)住院的高风险相关。因此,需要新的工具来早期识别具有高风险特征的患者。心脏磁共振成像(CMR)进行的区域应变评估在描述HF中的变形损害方面似乎更具优势。MyoHealth评分是一种有前景的早期识别心脏变化的工具。
招募了无论左心室射血分数(LVEF)如何的心力衰竭患者和无症状对照者,并获得了基于CMR的测量值。对于该分析,无症状对照组(n = 19)被分为无CV合并症或无心脏异常证据的无症状受试者(n = 12)和有CV合并症或有心脏异常证据的无症状受试者(n = 7)以及HFpEF患者(n = 19)。我们在静息状态和使用等长握力运动(HG)的负荷试验期间进行了CMR扫描。静息状态下评估MyoHealth评分显示,对照组左心室节段中85±9%的区域应变保留,有风险受试者中为73±11%,HFpEF患者中为73±8%。负荷试验期间,对照组的MyoHealth评分为84±7%,有风险受试者为83±7%,HFpEF患者为74±11%。
总之,我们首次表明,CV风险增加的无症状受试者在静息状态下表现出类似HFpEF的心肌变形受损,而在HG负荷试验下其结果与对照组相似。这组患者预防性治疗的潜力值得未来进一步研究。
[https://drks.de/search/de/trial/DRKS00015615],标识符[DRKS00015615]。