Bloemendal Niels T, Hertsig Richella, Benjamens Stan, van de Kuit Anouk, Swaab Tim, Yakar Derya, Minnee Robert C, Tielliu Ignace F J, Bakker Stephan J L, Pol Robert A
Department of Surgery, Division of Organ Transplantation, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands.
Department of Radiology, University of Groningen, University Medical Center Groningen, Groningen, The Netherlands.
Transplant Direct. 2023 Jan 12;9(2):e1435. doi: 10.1097/TXD.0000000000001435. eCollection 2023 Feb.
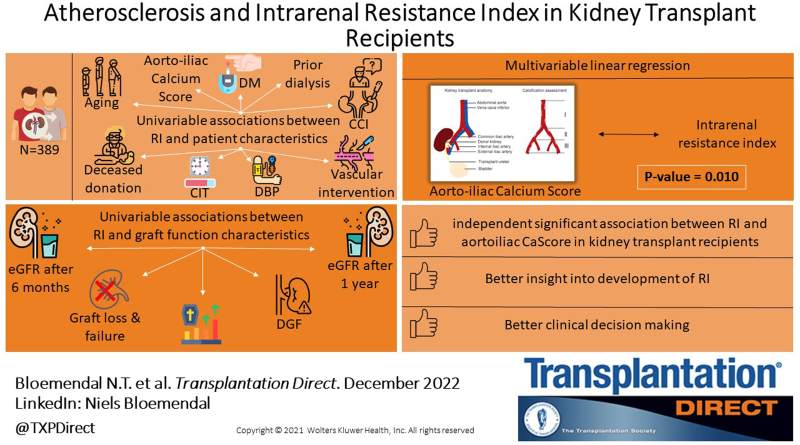
Atherosclerosis of the aortoiliac vessels can adversely affect kidney perfusion after kidney transplantation. Atherosclerosis severity can be determined using the calcium score (CaScore). Potential problems with posttransplantation kidney perfusion can be determined using the intrarenal resistance index (RI). This study investigated the association between aortoiliac CaScore and RI in kidney transplant recipients.
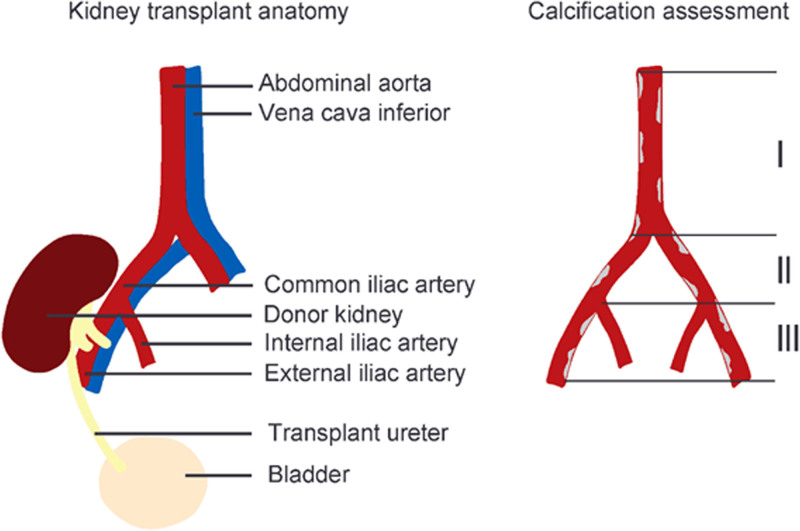
Kidney transplant recipients (2004-2019), for whom the CaScore and RI were determined, were included in this dual-center cohort study. CaScore was measured in 3 aortoiliac segments using noncontrast CT imaging. RI was determined using Doppler ultrasound. Multivariable linear regression analyses were performed between the CaScore and RI, adjusted for confounding variables.
The mean age of the 389 included patients was 59 (±13) y. The mean RI (unitless) was 0.71 (±0.09)' and the median CaScore (unitless) was 3340 (399-7833). In univariable linear regression analyses with RI as the dependent variable, CaScore ( = 0.011; < 0.001) was positively associated with RI. Moreover, recipient age ( = 0.014; < 0.001), history of diabetes ( = 0.029; = 0.003), recipient history of vascular interventions ( = 0.032; = 0.002), prior dialysis ( = 0.029; = 0.003), deceased donor transplantation ( = 0.042; < 0.001), donation after cardiac death ( = 0.036; = 0.001), an increase in cold ischemia time ( = 0.011; < 0.001), and the Comprehensive Complication Index ( = 0.006; = 0.002) were also positively associated with RI, whereas preoperative recipient diastolic blood pressure ( = -0.007; = 0.030) was inversely associated. In multivariable analyses, CaScore and RI remained significantly ( = 0.010) associated, independent of adjustment for potential confounders. Furthermore, in univariable linear regression analyses, multiple graft function characteristics were associated with RI.
A significant association was found between CaScore and RI, independent of adjustment for multiple potential confounding factors, leading to a better insight into the development and interpretation of RI. Aortoiliac atherosclerosis should be considered when interpreting the RI and determining the possible cause of malperfusion and graft failure after kidney transplantation.
腹主动脉髂动脉血管的动脉粥样硬化会对肾移植后的肾脏灌注产生不利影响。动脉粥样硬化的严重程度可以通过钙化积分(CaScore)来确定。移植后肾脏灌注的潜在问题可以通过肾内阻力指数(RI)来确定。本研究调查了肾移植受者腹主动脉髂动脉CaScore与RI之间的关联。
本双中心队列研究纳入了2004年至2019年期间测定了CaScore和RI的肾移植受者。使用非增强CT成像在3个腹主动脉髂动脉节段测量CaScore。使用多普勒超声确定RI。在对混杂变量进行调整后,对CaScore和RI进行多变量线性回归分析。
389例纳入患者的平均年龄为59(±13)岁。平均RI(无单位)为0.71(±0.09),CaScore中位数(无单位)为3340(399 - 7833)。在以RI为因变量的单变量线性回归分析中,CaScore(β = 0.011;P < 0.001)与RI呈正相关。此外,受者年龄(β = 0.014;P < 0.001)、糖尿病史(β = 0.029;P = 0.003)、受者血管介入史(β = 0.032;P = 0.002)、既往透析史(β = 0.029;P = 0.003)、 deceased供体移植(β = 0.042;P < 0.001)、心脏死亡后捐赠(β = 0.036;P = 0.001)、冷缺血时间增加(β = 0.011;P < 0.001)以及综合并发症指数(β = 0.006;P = 0.002)也与RI呈正相关,而术前受者舒张压(β = -0.007;P = 0.030)与RI呈负相关。在多变量分析中,CaScore和RI仍然显著(β = 0.010)相关,与潜在混杂因素的调整无关。此外,在单变量线性回归分析中,多种移植功能特征与RI相关。
在对多个潜在混杂因素进行调整后,发现CaScore与RI之间存在显著关联,这有助于更好地理解RI的发展和解读。在解释RI以及确定肾移植后灌注不良和移植失败的可能原因时,应考虑腹主动脉髂动脉粥样硬化。