Department of Psychiatry, Michigan State University, East Lansing, MI.
Directorate of Public Health and Environment, Kampala Capital City Authority, Kampala, Uganda.
Medicine (Baltimore). 2023 Jan 27;102(4):e32677. doi: 10.1097/MD.0000000000032677.
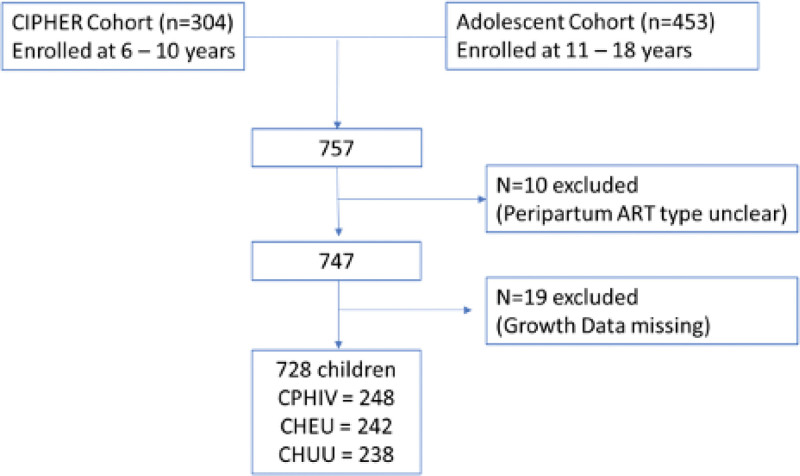
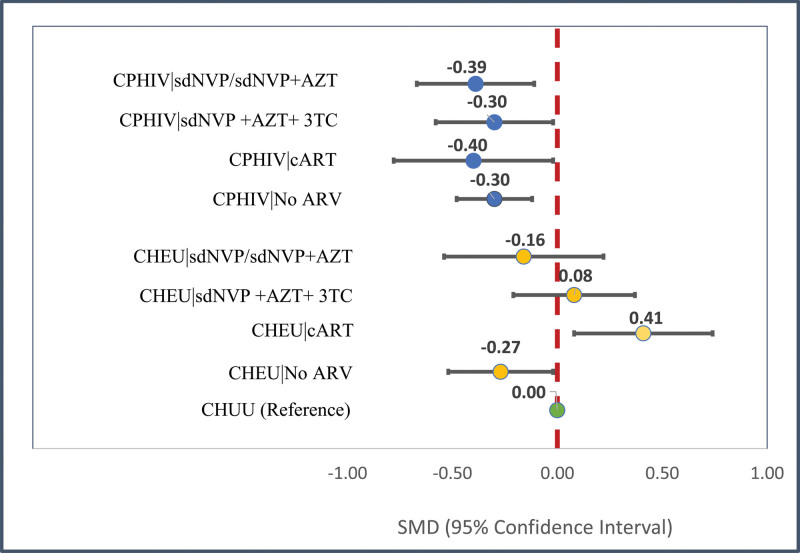
In utero/peripartum antiretroviral (IPA) drug exposure in human immunodeficiency virus (HIV)-exposed children has established benefit for prevention of HIV mother-to-child-transmission but its association with height-for-age by adolescence is unknown. Hence we quantify IPA-associated growth differences at 6 to 18 years old among children with perinatally acquired HIV (CPHIV) infection and children HIV exposed but uninfected (CHEU) relative to children HIV unexposed and uninfected (CHUU). Cohort study. Kampala, Uganda. Two hundred thirty eight community controls and 490 children of women living with HIV born between 2000 and 2011 in a community were enrolled at 6 to 18 years of age and followed every 6 months for 1 year. Height-for-age determined at enrollment, 6 and 12 months after enrollment using the World Health Organization reference. IPA exposure was retrospectively determined from medical records and categorized as: no IPA, single-dose nevirapine with/without zidovudine (sdNVP ± AZT), sdNVP + AZT + lamivudine, or combination antiretroviral therapy (cART). Mean differences (β) with 95% confidence intervals (CIs) in height-for-age over 12 months were evaluated according to IPA exposure for CPHIV and CHEU and relative to CHUU using longitudinal linear mixed effects models adjusted for caregiver factors (sex, age, education, functioning in caregiving role, and lifetime adversity) in Statistical Analysis Software (v.9.4). Regardless of IPA type, CPHIV grew worse than CHUU by school-age/adolescence (β = -0.30, 95% CI: -0.48, -0.11). Relative to CHUU height-for-age was similar for CHEU exposed to sdNVP ± AZT (β = -0.16, 95% CI: -0.46, 0.14) and for CHEU exposed to sdNVP + AZT + lamivudine (β = 0.08, 95% CI: -0.20, 0.35). However, CHEU without any IPA exposure had lower height-for-age (β = -0.27, 95% CI: -0.52, -0.00) whereas CHEU with cART exposure had greater height-for-age (β = 0.41, 95% CI: 0.10, 0.71) in comparison with CHUU by 6 to 18 years old. Our findings suggest that CHEU may achieve height-for-age parity with CHUU by school-age and adolescent years- especially if provided benefit of effective cART in the peripartum period. However, CPHIV regardless of IPA exposure type and CHEU without IPA exposure remain at a disadvantage and will benefit from intervention to support their growth.
在人类免疫缺陷病毒(HIV)暴露的儿童中,产前/围产期抗逆转录病毒(IPA)药物暴露对预防母婴传播 HIV 具有明确的益处,但它与青春期身高的关系尚不清楚。因此,我们在感染了围产期 HIV(CPHIV)的儿童和 HIV 暴露但未感染(CHEU)的儿童中,以及未感染 HIV 的儿童和未感染(CHUU)的儿童中,定量评估了 IPA 相关的生长差异,这些儿童是在 6 至 18 岁时接受评估的。队列研究。乌干达坎帕拉。在社区中,我们招募了 238 名社区对照和 490 名在社区中生活的 HIV 阳性妇女所生的儿童,他们在 6 至 18 岁时接受了登记,并在登记后 6 个月和 12 个月时每 6 个月进行一次随访,共随访 1 年。使用世界卫生组织参考标准,在登记时和登记后 6 个月和 12 个月时确定身高-年龄。从病历中回顾性确定 IPA 暴露情况,并分为以下几类:无 IPA、单次剂量奈韦拉平/齐多夫定(sdNVP±AZT)、sdNVP+AZT+拉米夫定或联合抗逆转录病毒治疗(cART)。使用纵向线性混合效应模型,根据 CPHIV 和 CHEU 的 IPA 暴露情况以及与 CHUU 的相对情况,评估 12 个月内身高-年龄的平均差异(β),并对 caregiver 因素(性别、年龄、教育、护理角色功能和终生逆境)进行调整,分析采用统计分析软件(v.9.4)。无论 IPA 类型如何,CPHIV 在学龄/青春期的生长状况都比 CHUU 差(β=-0.30,95%CI:-0.48,-0.11)。与 CHUU 相比,暴露于 sdNVP±AZT 的 CHEU(β=-0.16,95%CI:-0.46,0.14)和暴露于 sdNVP+AZT+拉米夫定的 CHEU(β=0.08,95%CI:-0.20,0.35)的身高-年龄相似。然而,未接受任何 IPA 暴露的 CHEU 的身高-年龄较低(β=-0.27,95%CI:-0.52,-0.00),而接受 cART 暴露的 CHEU 的身高-年龄较高(β=0.41,95%CI:0.10,0.71),与 6 至 18 岁的 CHUU 相比。我们的研究结果表明,CHEU 可能在学龄和青少年时期达到与 CHUU 相同的身高-年龄水平-尤其是如果在围产期提供有效的 cART 获益。然而,无论 IPA 暴露类型如何,CPHIV 和未接受 IPA 暴露的 CHEU 仍处于不利地位,需要采取干预措施来支持他们的生长。