van Husen Georg, Virdone Saverio, Pieper Karen, Kayani Gloria, Fox Keith A A
tenac.io, Oberwallstrasse 6, 10117 Berlin, Germany.
Department of Statistics, The Thrombosis Research Institute, London, UK.
Eur Heart J Digit Health. 2022 Mar 25;3(2):181-194. doi: 10.1093/ehjdh/ztac011. eCollection 2022 Jun.
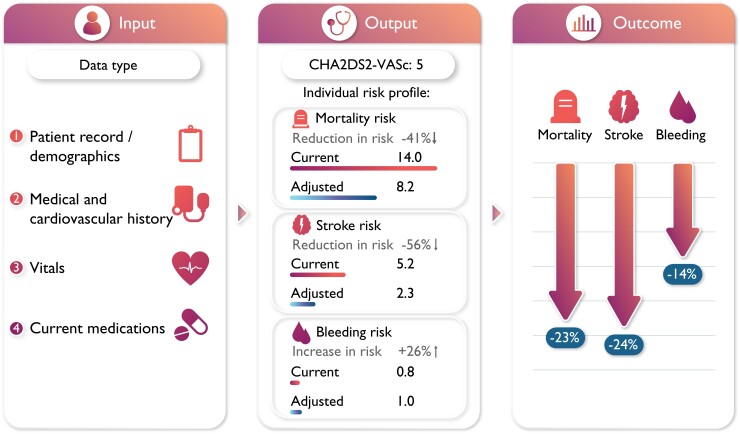
Atrial fibrillation (AF) management guidelines advise using risk tools to optimize AF treatment. This study aims to develop a dynamic and clinically applicable digital device to assess stroke and bleeding risk, and to facilitate outcome improvements in AF patients. The device will provide tailored treatment recommendations according to easily attainable individual patient data.
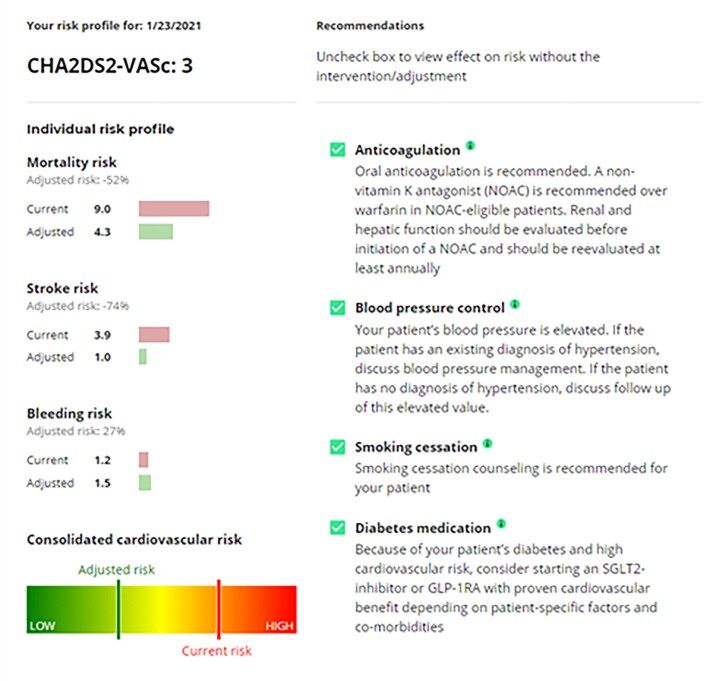
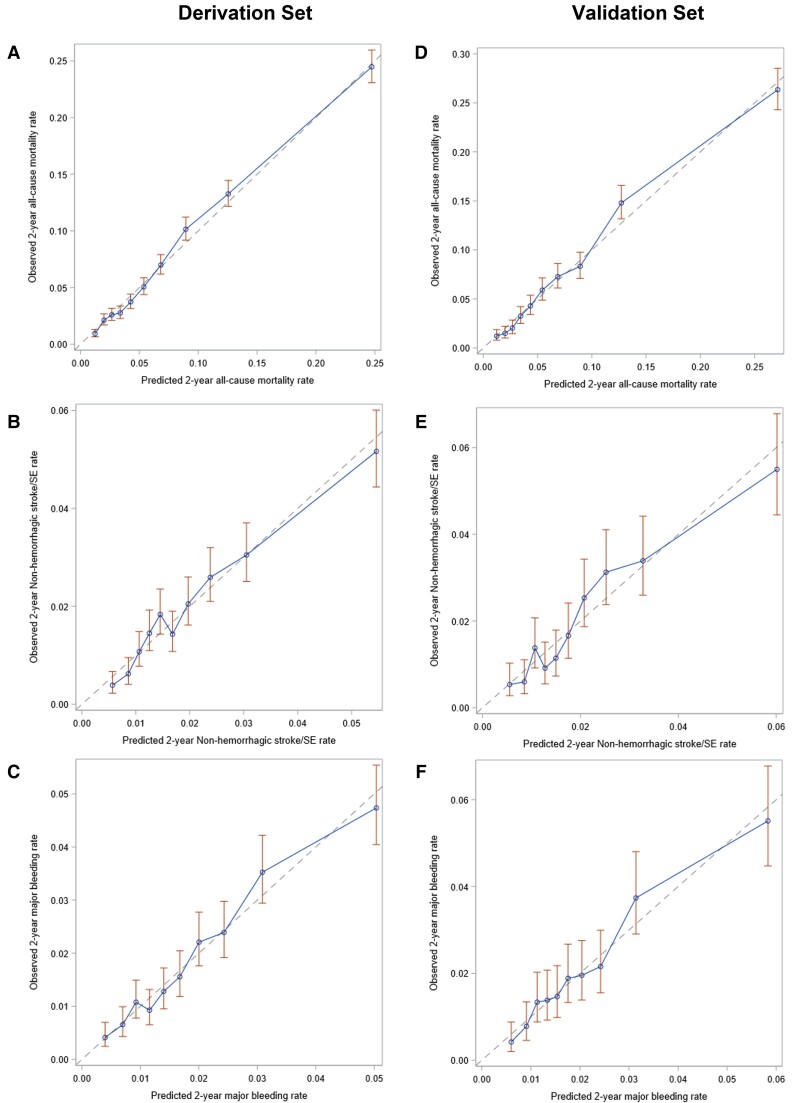
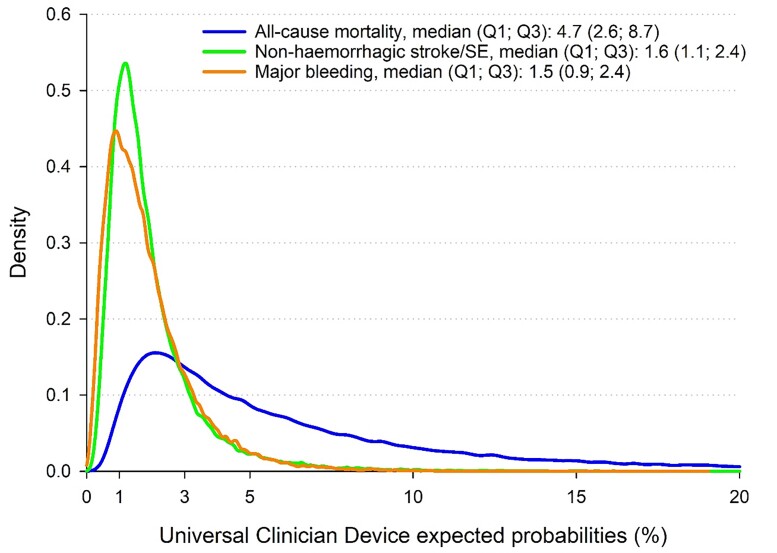
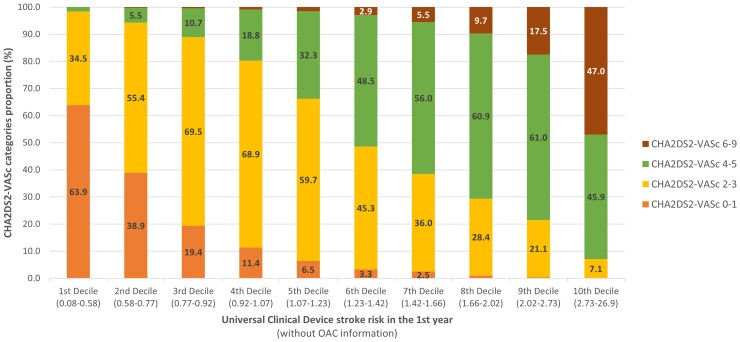
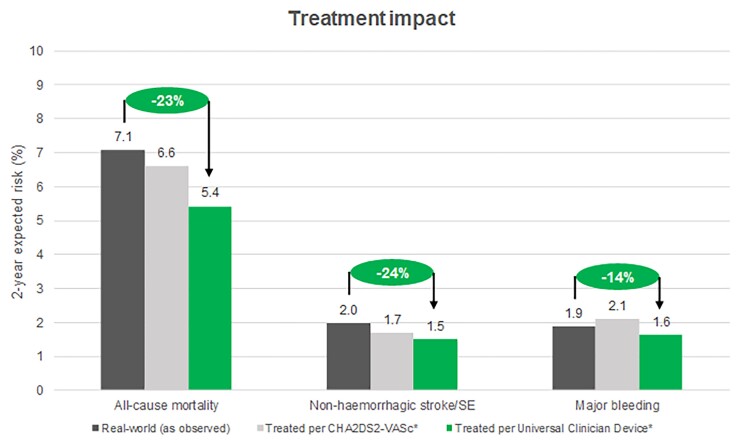
This Universal Clinician Device (UCD) was created using the GARFIELD-AF registry using a split sample approach. The GARFIELD-AF risk tool was adapted with two modifications. First, predictors with ≥1000 missing data points were separated, allowing expected risks estimation. Second, recommendations for modifiable risk factors and associated 2-year outcome estimates were incorporated. Outcomes of interest were all-cause mortality, non-haemorrhagic stroke/systemic embolism (SE), and major bleeding. All patients were randomized to a derivation ( = 34853) and validation cohort ( = 17165). In the derivation cohort, predictors were identified using least absolute shrinkage and selection operator regression. Cox models were fitted with the selected parameters. The UCD demonstrated superior predictive power compared with CHADSVASc for all-cause mortality [0.75(0.75-0.76) vs. 0.71(0.70-0.72)] and non-haemorrhagic stroke/SE [0.68(0.66-0.70) vs. 0.65(0.63-0.67)], and with HAS-BLED for major bleeding [0.69(0.67-0.71) vs. 0.64(0.62-0.65)]. Universal Clinician Device recommendations reduced all-cause mortality (8.45-5.42%) and non-haemorrhagic stroke/SE (2.58-1.50%). Patients with concomitant diabetes and chronic kidney disease benefitted further, reducing mortality risk from 13.15% to 8.67%. One-third of patients with a CHADSVASc score of >1 had the lowest risk of stroke.
The UCD simultaneously predicts mortality, stroke, and bleeding risk in patients using easily attainable individual clinical data and guideline-based optimized treatment plans.
URL: http://www.clinicaltrials.gov. Unique identifier for GARFIELD-AF: NCT01090362.
心房颤动(AF)管理指南建议使用风险评估工具来优化AF治疗。本研究旨在开发一种动态且临床适用的数字设备,以评估中风和出血风险,并促进AF患者的治疗效果改善。该设备将根据易于获取的个体患者数据提供量身定制的治疗建议。
本通用临床医生设备(UCD)是利用GARFIELD-AF注册研究,采用拆分样本法创建的。对GARFIELD-AF风险评估工具进行了两项修改。首先,将缺失数据点≥1000的预测因素分离出来,以便进行预期风险估计。其次,纳入了针对可改变风险因素的建议以及相关的2年预后估计。感兴趣的结局指标为全因死亡率、非出血性中风/全身性栓塞(SE)和大出血。所有患者被随机分为推导队列(n = 34853)和验证队列(n = 17165)。在推导队列中,使用最小绝对收缩和选择算子回归确定预测因素。用选定的参数拟合Cox模型。与CHADSVASc相比,UCD在全因死亡率[0.75(0.75 - 0.76)对0.71(0.70 - 0.72)]和非出血性中风/SE[0.68(0.66 - 0.70)对0.65(0.63 - 0.67)]方面显示出更好的预测能力,与HAS-BLED相比,在大出血方面也有更好的预测能力[0.69(0.67 - 0.71)对0.64(0.62 - 0.65)]。通用临床医生设备的建议降低了全因死亡率(8.45% - 5.42%)和非出血性中风/SE(2.58% - 1.50%)。合并糖尿病和慢性肾脏病的患者获益更大,将死亡风险从13.15%降至8.67%。CHADSVASc评分>1的患者中有三分之一的中风风险最低。
UCD使用易于获取的个体临床数据和基于指南的优化治疗方案,同时预测患者的死亡率、中风和出血风险。
网址:http://www.clinicaltrials.gov。GARFIELD-AF的唯一标识符:NCT01090362。