Institute of Applied Health Research, University of Birmingham, Birmingham, UK; Warwick Medical School, University of Warwick, Coventry, UK.
Faculty of Medicine, University of Alcala, Madrid, Spain.
Br J Gen Pract. 2023 Oct 26;73(736):e816-e824. doi: 10.3399/BJGP.2023.0082. Print 2023 Nov.
The GARFIELD-AF tool is a novel risk tool that simultaneously assesses the risk of all-cause mortality, stroke or systemic embolism, and major bleeding in patients with atrial fibrillation (AF).
To validate the GARFIELD-AF tool using UK primary care electronic records.
A retrospective cohort study using the Clinical Practice Research Datalink (CPRD) linked with Hospital Episode Statistics data and Office for National Statistics mortality data.
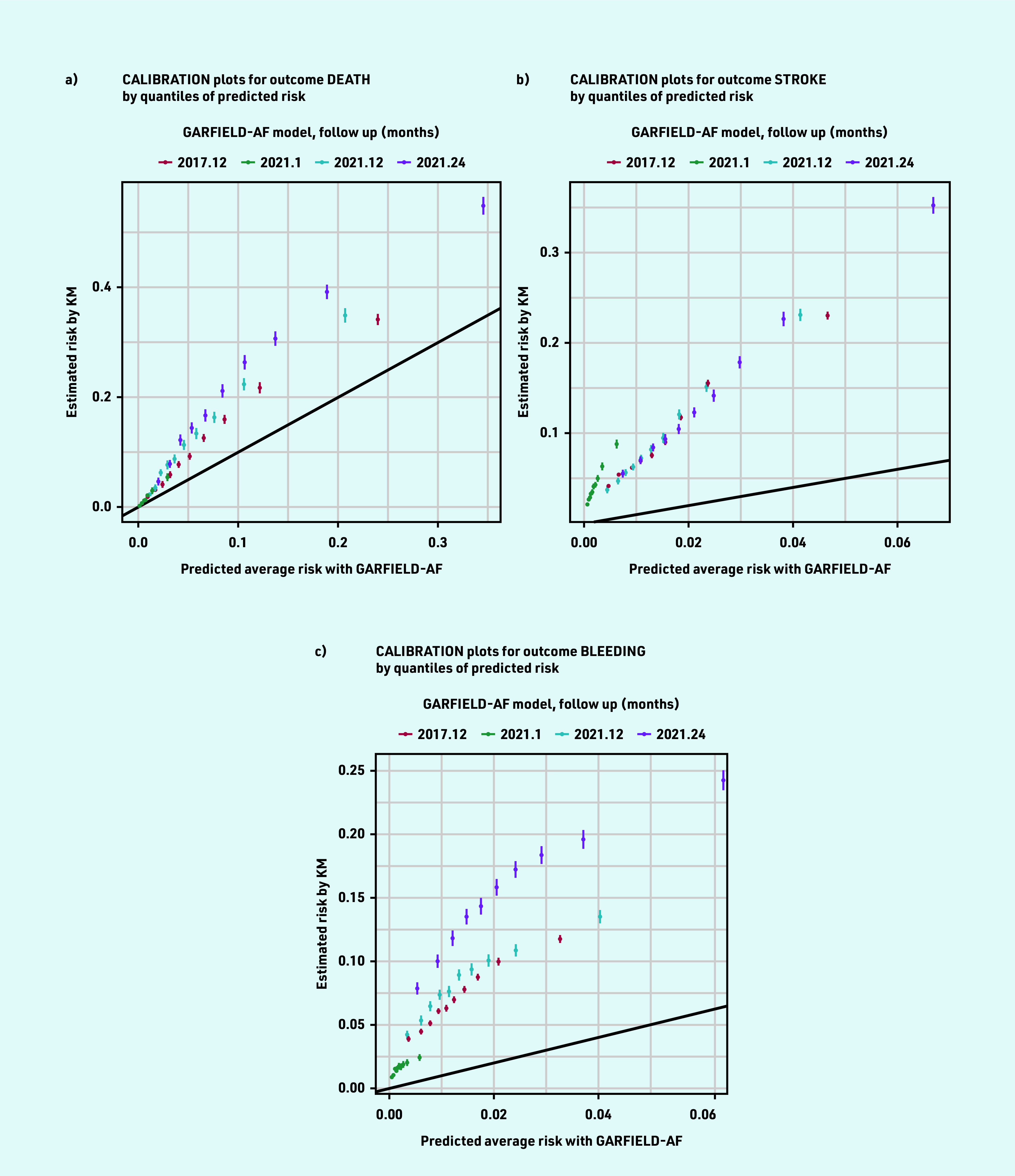
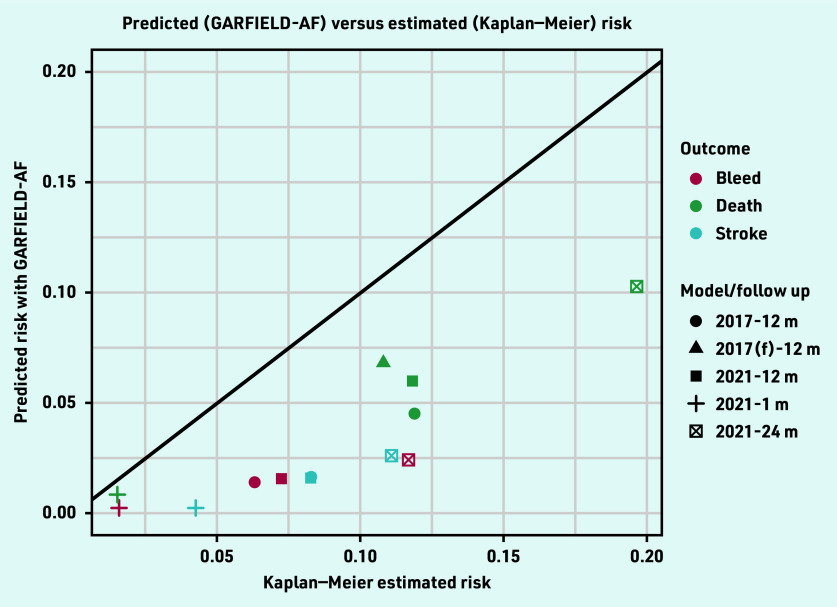
Discrimination was evaluated using the area under the curve (AUC) and calibration was evaluated using calibration-in-the-large regression and calibration plots.
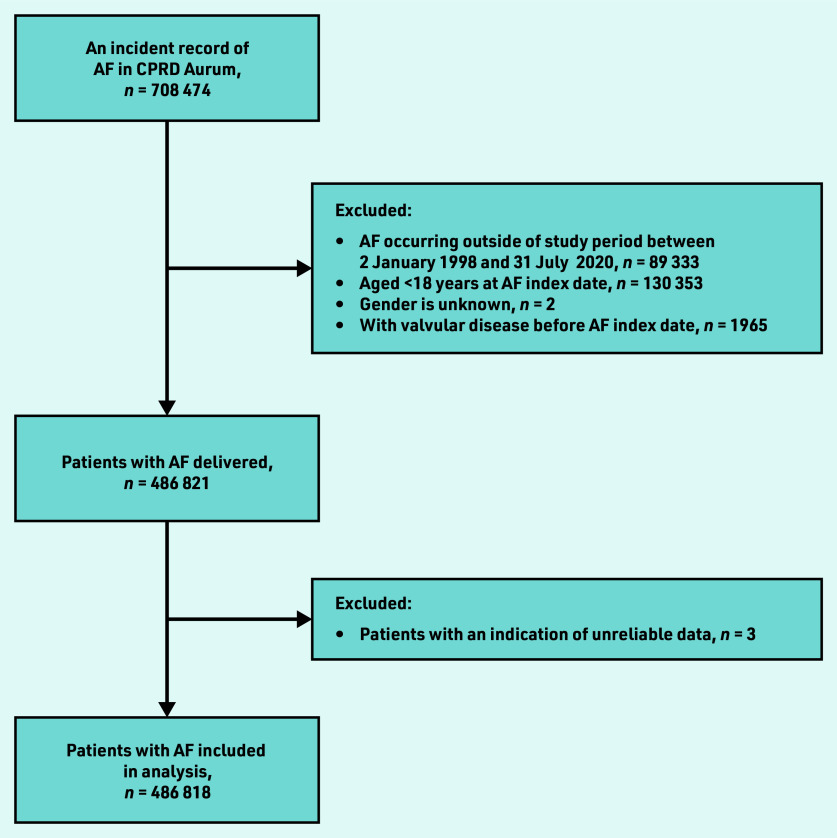
A total of 486 818 patients aged ≥18 years with incident diagnosis of non-valvular AF between 2 January 1998 and 31 July 2020 were included; 50.6% ( = 246 425/486 818) received anticoagulation at diagnosis The GARFIELD- AF models outperformed the CHADSVASc and HAS-BLED scores in discrimination ability of death, stroke, and major bleeding at all the time points. The AUC for events at 1 year for the 2017 models were: death 0.747 (95% confidence interval [CI] = 0.744 to 0.751) versus 0.635 (95% CI = 0.631 to 0.639) for CHADSVASc; stroke 0.666 (95% CI = 0.663 to 0.669) versus 0.625 (95% CI = 0.622 to 0.628) for CHADSVASc; and major bleeding 0.602 (95% CI = 0.598 to 0.606) versus 0.558 (95% CI = 0.554 to 0.562) for HAS- BLED. Calibration between predicted and Kaplan- Meier observed events was inadequate with the GARFIELD-AF models.
The GARFIELD-AF models were superior to the CHADSVASc score for discriminating stroke and death and superior to the HAS-BLED score for discriminating major bleeding. The models consistently underpredicted the level of risk, suggesting that a recalibration is needed to optimise its use in the UK population.
GARFIELD-AF 工具是一种新颖的风险工具,可同时评估心房颤动(AF)患者的全因死亡率、卒中和全身性栓塞以及大出血的风险。
使用英国初级保健电子记录验证 GARFIELD-AF 工具。
一项回顾性队列研究,使用临床实践研究数据链接(CPRD)与医院入院统计数据和国家统计局死亡率数据链接。
使用曲线下面积(AUC)评估区分度,并使用大校准回归和校准图评估校准。
共纳入 1998 年 1 月 2 日至 2020 年 7 月 31 日期间诊断为非瓣膜性 AF 的年龄≥18 岁的 486818 例患者;50.6%(=246425/486818)在诊断时接受抗凝治疗。GARFIELD-AF 模型在所有时间点的死亡、卒中和大出血的判别能力均优于 CHADSVASc 和 HAS-BLED 评分。2017 年模型的 1 年事件 AUC 为:死亡 0.747(95%置信区间[CI] = 0.744 至 0.751),CHADSVASc 为 0.635(95%CI = 0.631 至 0.639);卒中 0.666(95%CI = 0.663 至 0.669),CHADSVASc 为 0.625(95%CI = 0.622 至 0.628);大出血 0.602(95%CI = 0.598 至 0.606),HAS-BLED 为 0.558(95%CI = 0.554 至 0.562)。GARFIELD-AF 模型的预测与 Kaplan-Meier 观察到的事件之间的校准不足。
GARFIELD-AF 模型在区分卒中和死亡方面优于 CHADSVASc 评分,在区分大出血方面优于 HAS-BLED 评分。该模型始终低估风险水平,表明需要重新校准以优化其在英国人群中的使用。