Department of Endocrinology, Hospital del Tajo, Madrid, Spain.
Department of Endocrinology, Hospital Universitario de Toledo, Toledo, Spain.
Front Endocrinol (Lausanne). 2023 Jan 13;13:1071775. doi: 10.3389/fendo.2022.1071775. eCollection 2022.
The dynamic risk stratification (DRS) is a relatively new system in thyroid cancer that considers the response to primary treatment to improve the initial risk of recurrence. We wanted to validate DRS system in a nationwide multicenter study and explore if the incorporation of BRAFV600E into DRS helps to better categorize and predict outcomes.
Retrospective study of 685 patients from seven centers between 1991 and 2016, with a mean age of 48 years and a median follow-up time of 45 months (range 23-77). The overall BRAFV600E prevalence was 53.4%. We classified patients into four categories based on DRS ('excellent', 'indeterminate', 'biochemical incomplete', and 'structural incomplete' response). Cox regression was used to calculate adjusted hazard ratios (AHR) and proportions of variance explained (PVEs).
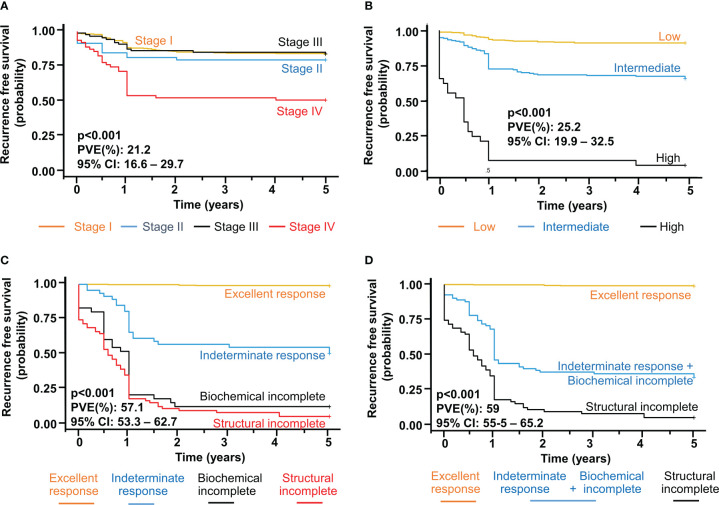
We found 21.6% recurrences and 2.3% cancer-related deaths. The proportion of patients that developed recurrence in excellent, indeterminate, biochemical incomplete and structural incomplete response to therapy was 1.8%, 54%, 91.7% and 96.2% respectively. Considering the outcome at the end of the follow up, patients showed no evidence of disease (NED) in 98.2, 52, 33.3 and 25.6% respectively. Patients in the structural incomplete category were the only who died (17.7%). Because they have similar outcomes in terms of NED and survival, we integrated the indeterminate and biochemical incomplete response into one unique category creating the 3-tiered DRS system. The PVEs of the AJCC/TNM staging, ATA risk classification, 4-tiered DRS, and 3-tiered DRS to predict recurrence at five years were 21%, 25%, 57% and 59% respectively. BRAFV600E was significantly associated with biochemical incomplete response (71.1 vs 28.9%) (HR 2.43; 95% CI, 1.21 to 5.23; p=0.016), but not with structural incomplete response or distant metastases. BRAF status slightly changes the AHR values of the DRS categories but is not useful for different risk grouping.
This is the first multicenter study to validate the 4-tiered DRS system. Our results also show that the 3-tiered DRS system, by integrating indeterminate and biochemical incomplete response into one unique category, may simplify response to therapy keeping the system accurate. BRAF status does not provide any additional benefit to DRS.
动态风险分层(DRS)是甲状腺癌的一个相对较新的系统,它考虑了对初始治疗的反应,以改善复发的初始风险。我们希望在一项全国多中心研究中验证 DRS 系统,并探讨 BRAFV600E 的纳入是否有助于更好地分类和预测结果。
对 1991 年至 2016 年间来自七个中心的 685 例患者进行回顾性研究,平均年龄为 48 岁,中位随访时间为 45 个月(范围为 23-77 个月)。整体 BRAFV600E 的流行率为 53.4%。我们根据 DRS 将患者分为四类(“优秀”、“不确定”、“生化不完全”和“结构不完全”反应)。使用 Cox 回归计算调整后的危险比(AHR)和方差解释比例(PVE)。
我们发现 21.6%的患者复发,2.3%的患者死于癌症。在治疗后表现出“优秀”、“不确定”、“生化不完全”和“结构不完全”反应的患者中,分别有 1.8%、54%、91.7%和 96.2%的患者出现复发。考虑到随访结束时的结果,98.2%、52%、33.3%和 25.6%的患者分别为无疾病证据(NED)。只有结构不完全组的患者死亡(17.7%)。由于他们在 NED 和生存方面的结果相似,我们将不确定和生化不完全的反应整合为一个独特的类别,创建了 3 级 DRS 系统。AJCC/TNM 分期、ATA 风险分类、4 级 DRS 和 3 级 DRS 预测 5 年内复发的 PVE 分别为 21%、25%、57%和 59%。BRAFV600E 与生化不完全反应显著相关(71.1%与 28.9%)(HR 2.43;95%CI,1.21 至 5.23;p=0.016),但与结构不完全反应或远处转移无关。BRAF 状态略微改变了 DRS 类别的 AHR 值,但对不同的风险分组没有帮助。
这是第一项验证 4 级 DRS 系统的多中心研究。我们的结果还表明,通过将不确定和生化不完全的反应整合为一个独特的类别,3 级 DRS 系统可以简化治疗反应,同时保持系统的准确性。BRAF 状态并不能为 DRS 提供任何额外的益处。