Department of International Health and Sustainable Development, Tulane University School of Public Health and Tropical Medicine, 1440 Canal St, Suite 2200, New Orleans, LA, 70112, USA.
Department of Health Policy and Management, Tulane University School of Public Health and Tropical Medicine, 1440 Canal St, Suite 1900, New Orleans, LA, 70112, USA.
Reprod Health. 2023 Jan 30;20(1):24. doi: 10.1186/s12978-023-01571-6.
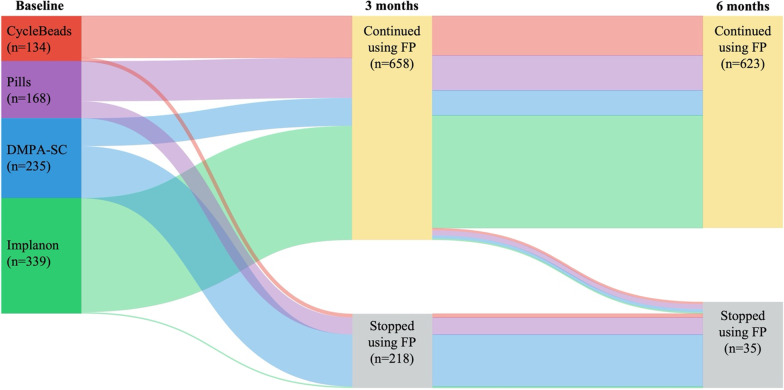
While community-based interventions are a proven high-impact strategy to increase contraceptive uptake in low-income countries, their capacity to support women's contraceptive choices (including continued use, switching and discontinuation) in the long run remains insufficiently discussed. This cohort study follows 883 women 3 and 6 months after they received a modern method during community campaigns organized in Kinshasa (D.R. Congo), to analyze their contraceptive trajectories and the factors associated with ever discontinuing contraceptive use in the first 6 months following a campaign. In the community-based distribution (CBD) model currently institutionalized in DRC, campaign clients are not provided with additional doses or support, besides baseline counseling, to (dis-)continue using the method they received, but must rely on Family Planning resources within the existing local health system. Almost a third (28.9%) of all women discontinued modern contraception during the study period, with much higher discontinuation rates for short-acting methods (38.7% for pills and up to 68.9% for DMPA-SC). Variables previously associated with high discontinuation (marital status, fertility intentions and side-effects) led to higher odds of "ever discontinuing". However, these variables became non-significant when controlling for resupply issues. Women's self-reported reasons for discontinuation confirmed the multivariate regression results. Detailed sub-analysis of resupply issues for pills, injectables and Cyclebeads pointed to the role of cost, unreliable campaign schedules and weak integration of community-based strategies into the formal health system. Extremely low rates of implants removal suggest similar access to FP services issues. The study highlights the need to identify CBD strategies best suited to support women's choices and preferences towards successful contraceptive trajectories in fragile health systems.
虽然基于社区的干预措施是在低收入国家提高避孕措施使用率的一种经过验证的高影响力策略,但它们在长期内支持妇女做出避孕选择(包括继续使用、转换和停止使用)的能力仍未得到充分讨论。本队列研究随访了 883 名在金沙萨(刚果民主共和国)组织的社区活动中接受现代避孕方法的女性,以分析她们的避孕轨迹以及与在活动后前 6 个月内停止使用避孕措施相关的因素。在刚果民主共和国目前制度化的基于社区的分配(CBD)模式中,除了基线咨询外,社区活动中提供的方法不提供额外的剂量或支持来(停止)使用所接受的方法,而必须依靠现有当地卫生系统中的计划生育资源。在研究期间,几乎三分之一(28.9%)的所有女性停止了现代避孕措施,短期方法(避孕药的停药率为 38.7%,DMPA-SC 高达 68.9%)的停药率更高。先前与高停药率相关的变量(婚姻状况、生育意愿和副作用)导致“停止使用”的可能性更高。然而,当控制供应问题时,这些变量变得没有意义。女性对停药的自我报告原因证实了多元回归结果。对药丸、注射剂和 Cyclebeads 的供应问题的详细子分析表明,成本、不可靠的活动时间表以及将基于社区的策略纳入正式卫生系统的薄弱整合是导致问题的原因。植入物取出率极低表明类似的计划生育服务问题。该研究强调了需要确定最适合支持妇女选择和偏好的 CBD 策略,以实现脆弱卫生系统中的成功避孕轨迹。