Department of Cardiology, People's Hospital of Zhengzhou University, Henan Provincial People's Hospital, Zhengzhou University Central China Fuwai Hospital, No. 1 Fuwai Avenue, Zhengdong New District, Zhengzhou, Henan Province, China.
Henan Provincial Key Lab for Control of Coronary Heart Disease, Zhengzhou University Central China Fuwai Hospital, People's Hospital of Zhengzhou University, Zhengzhou, Henan Province, China.
BMC Cardiovasc Disord. 2023 Feb 2;23(1):61. doi: 10.1186/s12872-023-03099-w.
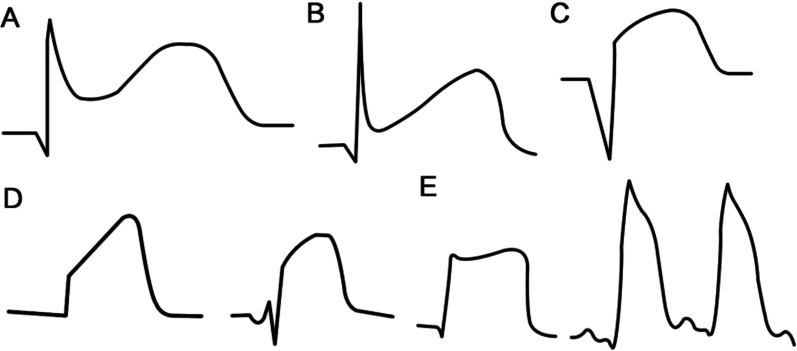
ST-segment elevation (STE) represents a repolarization dispersion marker underlying arrhythmogenesis in ST-segment elevation myocardial infarction (STEMI); however, its value for predicting malignant ventricular arrhythmia events (MVAEs) remains uncertain.
In total, 285 patients with STEMI and those with or without MVAEs who presented within 6 h of symptom onset were enrolled. The relationships between STE and clinical characteristics of MVAEs (defined as ventricular tachycardia or ventricular fibrillation) were analyzed using t-test, chi-square test, binary multivariate logistic regression, and receiver operating characteristic curve analysis.
Patients with STEMI and MVAEs had a shorter time from symptom onset to balloon time (p = 0.0285) and greater STE (p < 0.01) than those without MVAEs. The symptom-to-balloon time, age, and STE were associated with MVAEs after stepwise regression analysis in all cases. Only STE was significantly associated with the occurrence of MVAEs (all, p < 0.01). The area under the curve (AUC) of STE for predicting MVAEs was 0.905, and the cut-off value was 4.5 mV. When only infarct-related arteries were included in the analysis, the AUC of the left anterior descending artery was 0.925 with a cut-off value of 4.5 mV, that of the right coronary artery was 0.915 with a cut-off value of 4.5 mV, and that of the left circumflex artery was 0.929 with a cut-off value of 4.0 mV.
In patients with STEMI presenting within 6 h of symptom onset, age, symptom-to-balloon time, and STE were the main predictors for MVAEs. However, among these, STE was the strongest predictor for MVAEs and was an index for repolarization dispersion of cardiomyocytes in infarcted and non-infarcted areas.
ST 段抬高(STE)代表 ST 段抬高型心肌梗死(STEMI)中心律失常发生的复极离散标志物;然而,其预测恶性室性心律失常事件(MVAEs)的价值仍不确定。
共纳入 285 例 STEMI 患者,其中包括在症状发作后 6 小时内出现 MVAEs 和无 MVAEs 的患者。使用 t 检验、卡方检验、二元多变量逻辑回归和受试者工作特征曲线分析,分析 STE 与 MVAEs(定义为室性心动过速或心室颤动)的临床特征之间的关系。
与无 MVAEs 的患者相比,STEMI 合并 MVAEs 的患者从症状发作到球囊时间更短(p=0.0285),STE 更大(p<0.01)。在所有患者的逐步回归分析中,症状至球囊时间、年龄和 STE 与 MVAEs 相关。仅 STE 与 MVAEs 的发生显著相关(所有,p<0.01)。STE 预测 MVAEs 的曲线下面积(AUC)为 0.905,截值为 4.5 mV。当仅分析梗死相关动脉时,左前降支的 AUC 为 0.925,截值为 4.5 mV,右冠状动脉的 AUC 为 0.915,截值为 4.5 mV,左回旋支的 AUC 为 0.929,截值为 4.0 mV。
在症状发作后 6 小时内就诊的 STEMI 患者中,年龄、症状至球囊时间和 STE 是 MVAEs 的主要预测因素。然而,在这些因素中,STE 是 MVAEs 的最强预测因子,是梗死区和非梗死区心肌复极离散的指标。