Clinical Physiology, Department of Clinical Sciences LundFaculty of Medicine, Lund University, Box 117 221 00 Lund, Sweden.
Skåne University Hospital, Carl-Bertil Laurells gata 9, 214 28 Malmö, Sweden.
Cardiovasc Res. 2023 Oct 16;119(12):2230-2243. doi: 10.1093/cvr/cvad028.
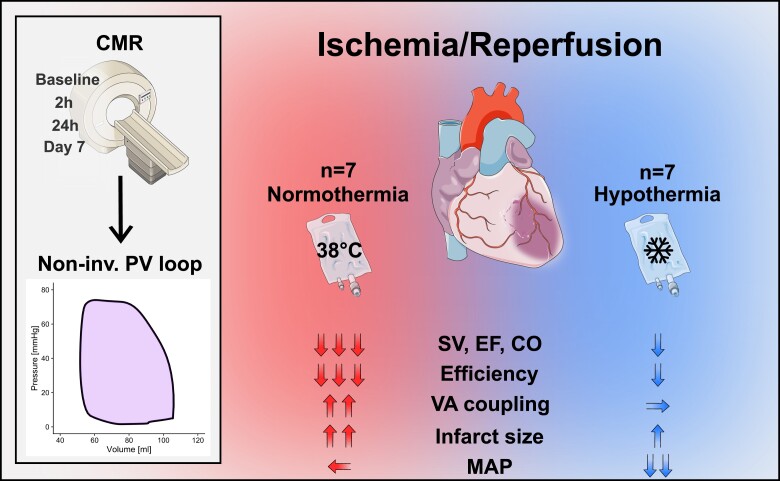
Mild hypothermia, 32-35°C, reduces infarct size in experimental studies, potentially mediating reperfusion injuries, but human trials have been ambiguous. To elucidate the cardioprotective mechanisms of mild hypothermia, we analysed cardiac performance in a porcine model of ischaemia/reperfusion, with serial cardiovascular magnetic resonance (CMR) imaging throughout 1 week using non-invasive pressure-volume (PV) loops.
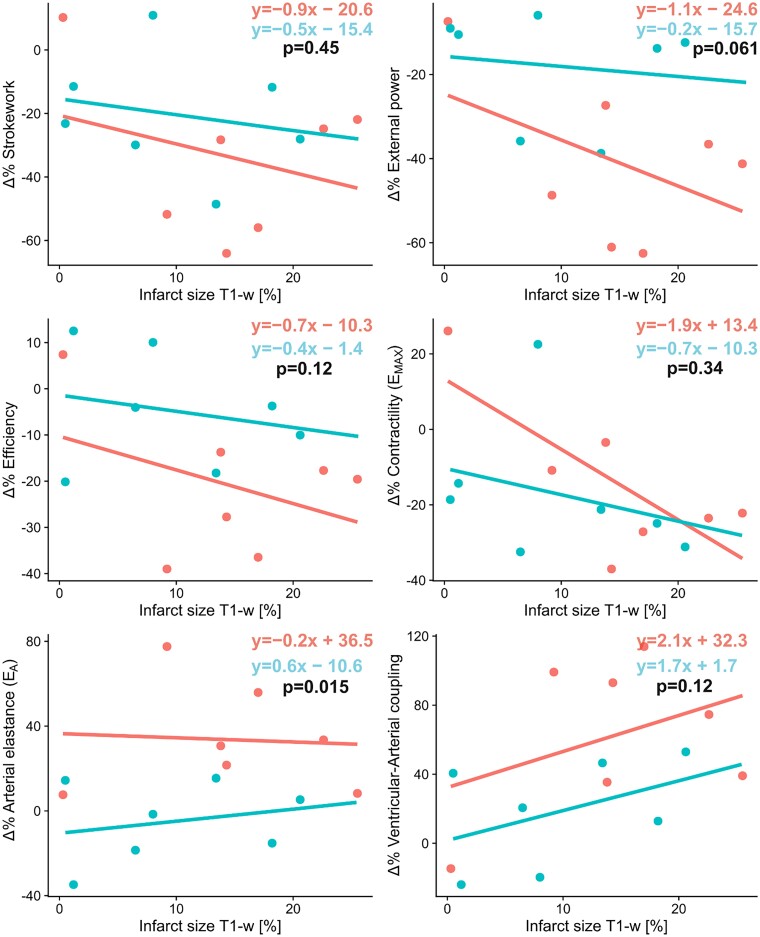
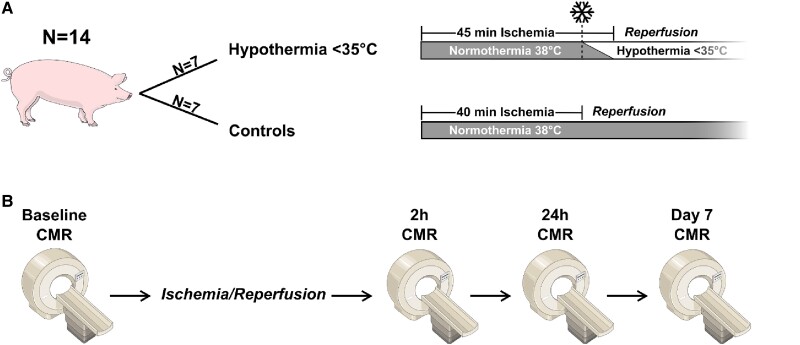
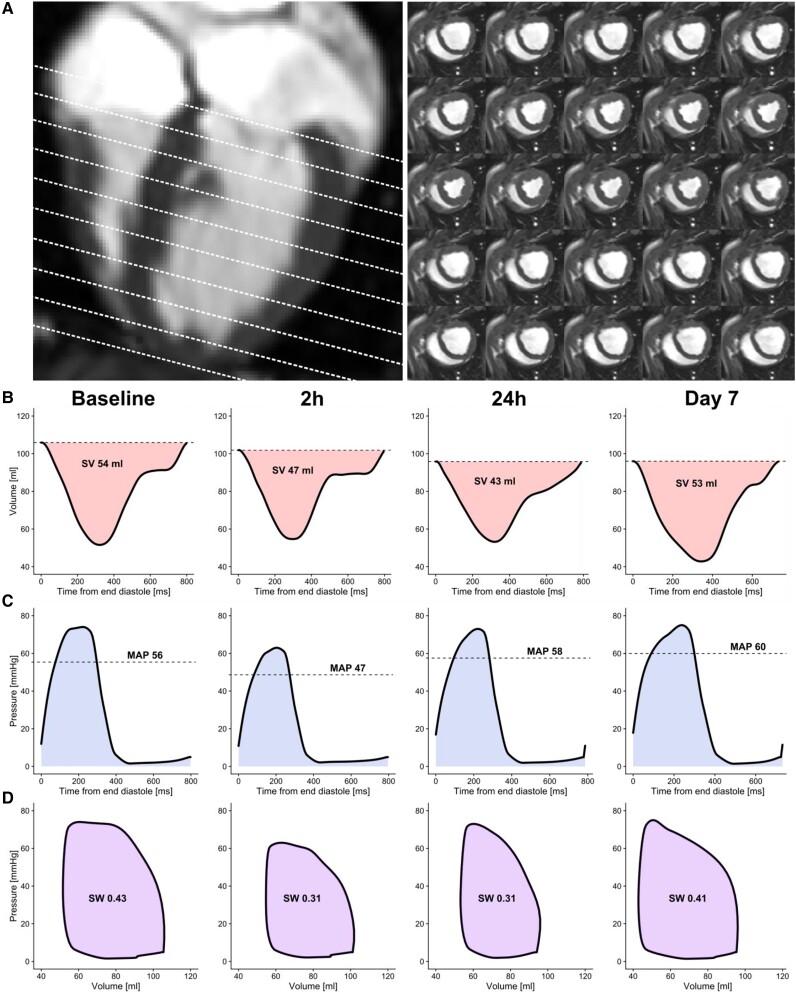
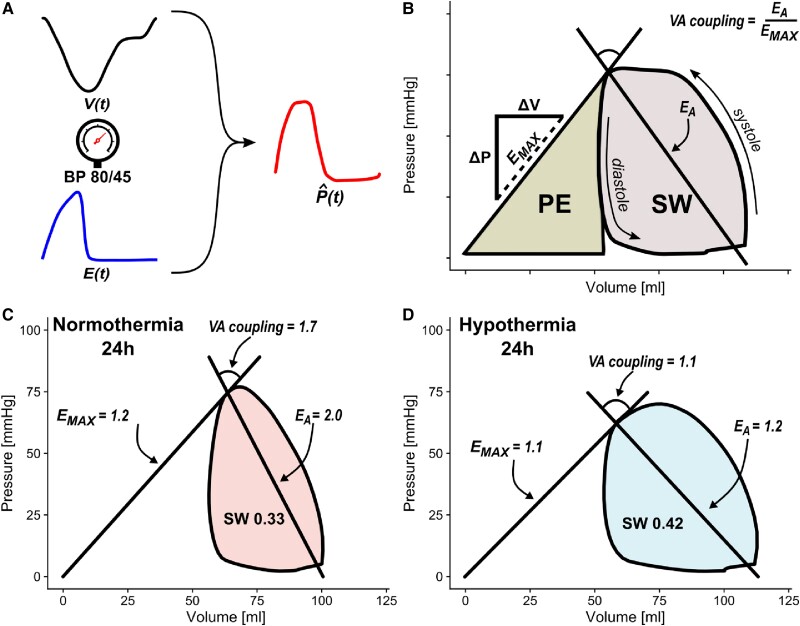
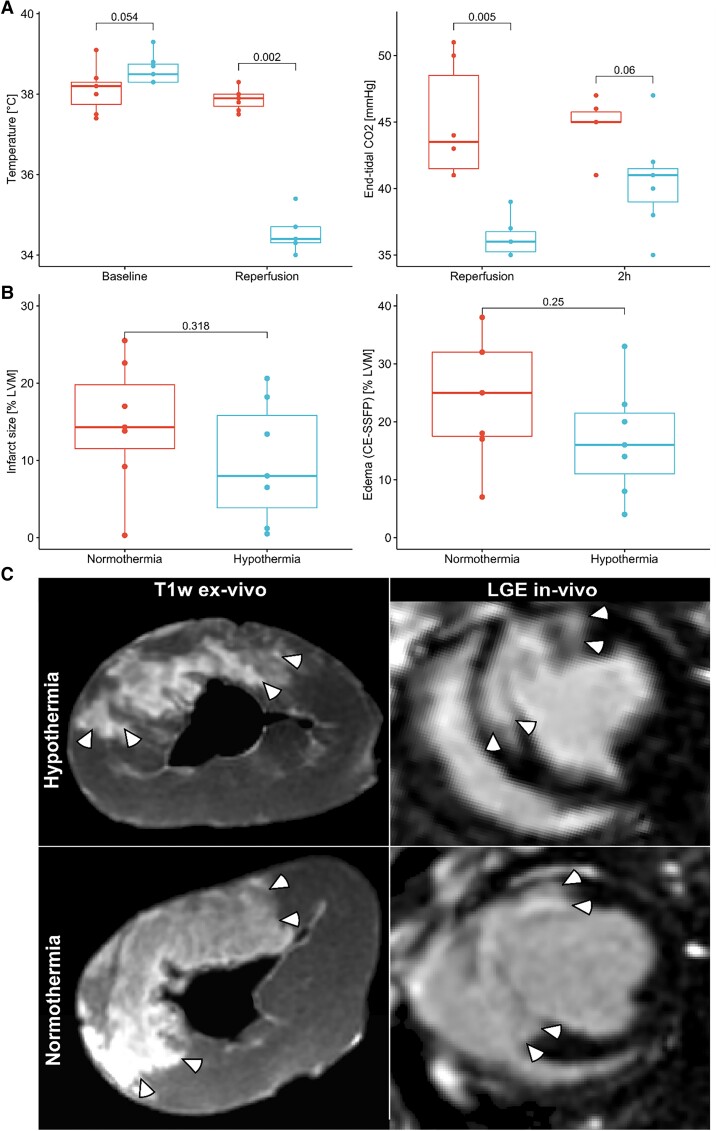
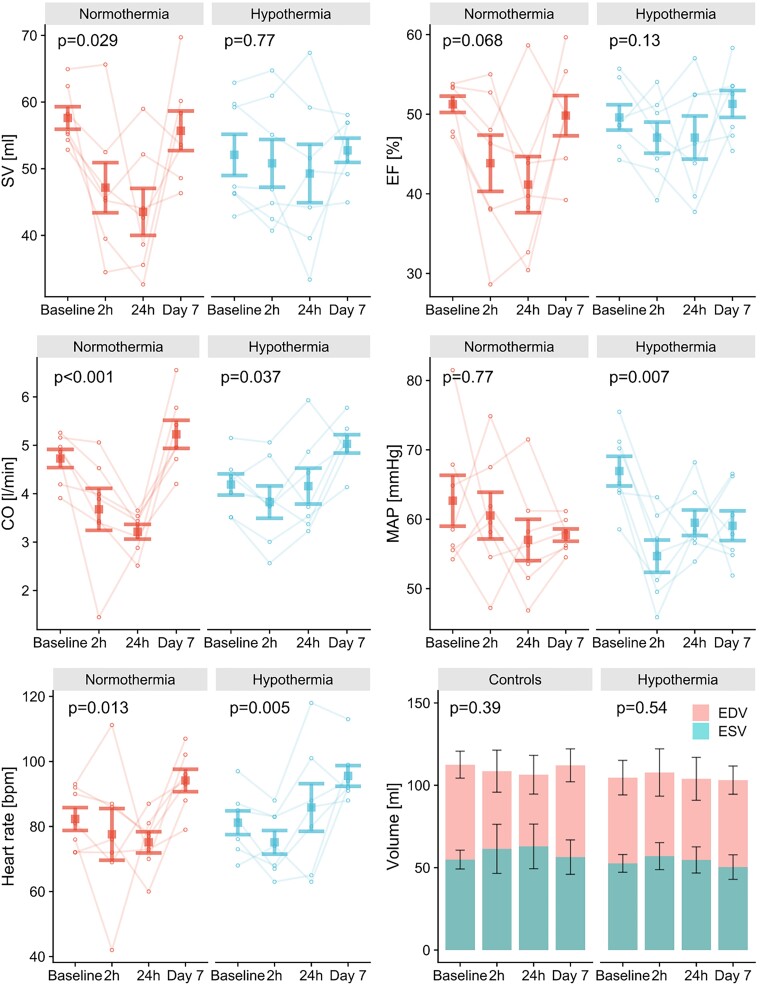
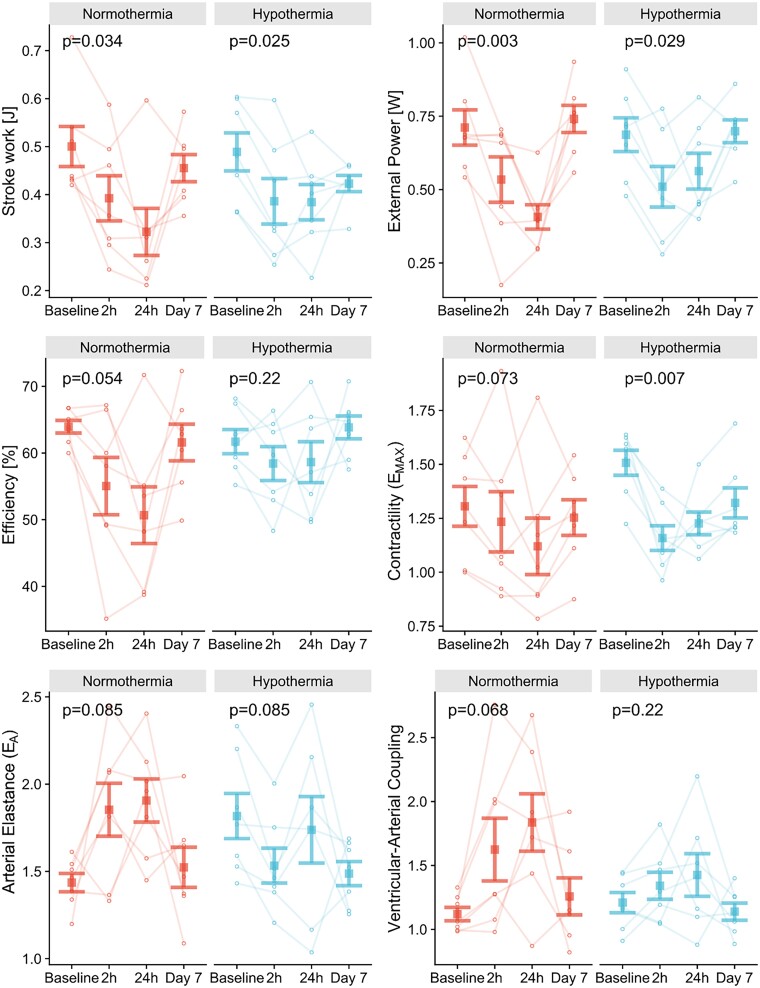
Normothermia and Hypothermia group sessions (n = 7 + 7 pigs, non-random allocation) were imaged with Cardiovascular magnetic resonance (CMR) at baseline and subjected to 40 min of normothermic ischaemia by catheter intervention. Thereafter, the Hypothermia group was rapidly cooled (mean 34.5°C) for 5 min before reperfusion. Additional CMR sessions at 2 h, 24 h, and 7 days acquired ventricular volumes and ischaemic injuries (unblinded analysis). Stroke volume (SV: -24%; P = 0.029; Friedmans test) and ejection fraction (EF: -20%; P = 0.068) were notably reduced at 24 h in the Normothermia group compared with baseline. In contrast, the decreases were ameliorated in the Hypothermia group (SV: -6%; P = 0.77; EF: -6%; P = 0.13). Mean arterial pressure remained stable in Normothermic animals (-3%, P = 0.77) but dropped 2 h post-reperfusion in hypothermic animals (-18%, P = 0.007). Both groups experienced a decrease and partial recovery pattern for PV loop-derived variables over 1 week, but the adverse effects tended to attenuate in the Hypothermia group. Infarct sizes were 10 ± 8% in Hypothermic and 15 ± 8% in Normothermic animals (P = 0.32). Analysis of covariance at 24 h indicated that hypothermia has cardioprotective properties incremental to reducing infarct size, such as higher external power (P = 0.061) and lower arterial elastance (P = 0.015).
Using non-invasive PV loops by CMR, we observed that mild hypothermia at reperfusion alleviates the heart's work after ischaemia/reperfusion injuries during the first week and preserves short-term cardiac performance. This hypothesis-generating study suggests hypothermia to have cardioprotective properties, incremental to reducing infarct size. The primary cardioprotective mechanism was likely an afterload reduction acutely unloading the left ventricle.
在实验研究中,轻度低温(32-35°C)可减少梗死面积,可能介导再灌注损伤,但人体试验结果并不明确。为了阐明轻度低温的心脏保护机制,我们通过连续的心血管磁共振(CMR)成像,在 1 周内使用非侵入性压力-容积(PV)环分析了缺血/再灌注猪模型的心脏功能。
在正常体温和低温组(n = 7 + 7 头猪,非随机分配)中,通过心血管磁共振(CMR)在基线时进行成像,并通过导管干预进行 40 分钟的正常体温缺血。此后,低温组迅速降温(平均 34.5°C)5 分钟,然后再灌注。在 2 小时、24 小时和 7 天的额外 CMR 会议中获取心室容积和缺血损伤(非盲分析)。与基线相比,在正常体温组中,24 小时时的每搏量(SV:-24%;P = 0.029;Friedmans 检验)和射血分数(EF:-20%;P = 0.068)明显降低。相比之下,低温组的降低幅度得到了改善(SV:-6%;P = 0.77;EF:-6%;P = 0.13)。在正常体温动物中,平均动脉压保持稳定(-3%,P = 0.77),但在低温动物中,再灌注后 2 小时下降(-18%,P = 0.007)。两组在 1 周内的 PV 环衍生变量均呈现下降和部分恢复的模式,但低温组的不良影响趋于减弱。低温组的梗死面积为 10±8%,正常体温组为 15±8%(P = 0.32)。24 小时的协方差分析表明,低温具有除减少梗死面积以外的心脏保护特性,如更高的外部功率(P = 0.061)和更低的动脉弹性(P = 0.015)。
通过 CMR 使用非侵入性的 PV 环,我们观察到,再灌注时的轻度低温可减轻缺血/再灌注损伤后心脏的工作负荷,并在第一周内保持短期的心脏功能。这项产生假说的研究表明,低温除了减少梗死面积外,还具有心脏保护特性。主要的心脏保护机制可能是急性减轻左心室后负荷,从而使左心室卸载。