Södertälje Hospital, Södertälje, Sweden.
Department of Anaesthesiology, Shaoxing People's Hospital, Shaoxing 312000, Zhejiang Province, PR of China.
Anaesthesiol Intensive Ther. 2022;54(5):369-377. doi: 10.5114/ait.2022.121003.
The mean systemic filling pressure (Pms) plays a central role for our understanding of the circulation. In a retrospective analysis of a clinical trial, we studied whether Pms indicates fluid responsiveness and whether Pms can indicate an anaesthesia-induced increase of the unstressed blood volume, which is the volume that does not increase the transmural pressure.
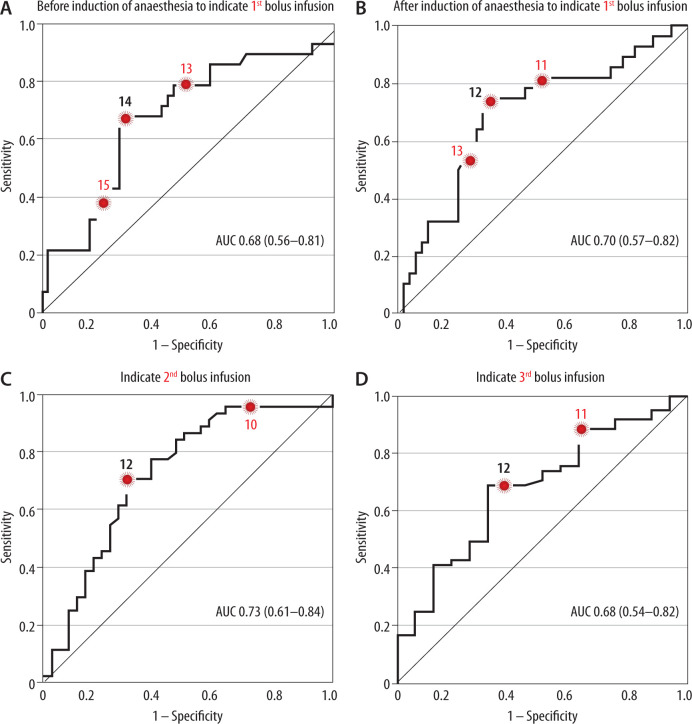
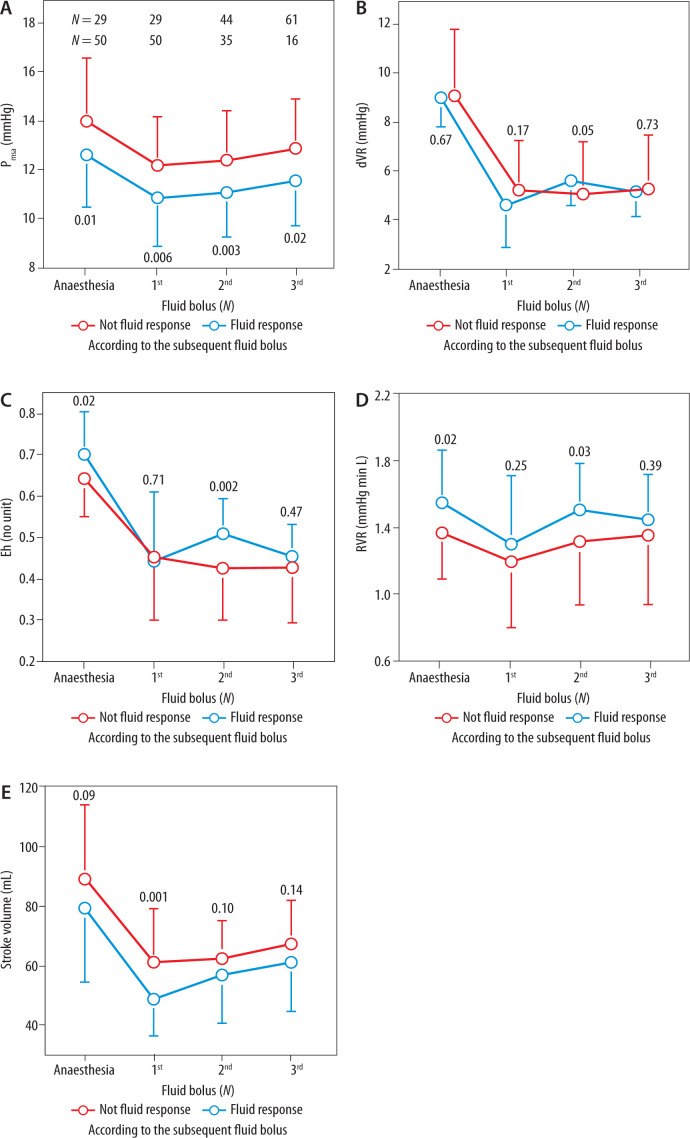
An analogue to P ms based on cardiac output, the mean arterial pressure and the central venous pressure, abbreviated to P msa , were calculated in 86 patients before induction of general anaesthesia and before 3 successive bolus infusions of 3 mL kg -1 of colloid fluid. An increase in stroke volume of ≥ 10% from a bolus infusion indicated fluid responsiveness. Receiver operator characteristic (ROC) curves were used to find the optimal cut-off for P msa to indicate fluid responsiveness. Changes in blood volume were estimated from anthropometric data and the haemodilution.
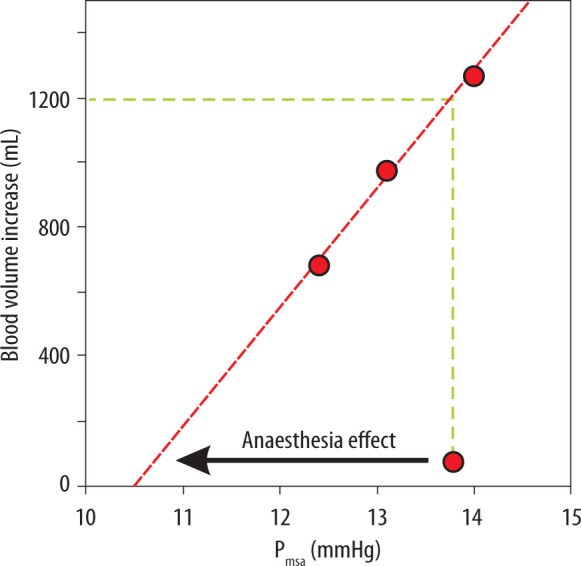
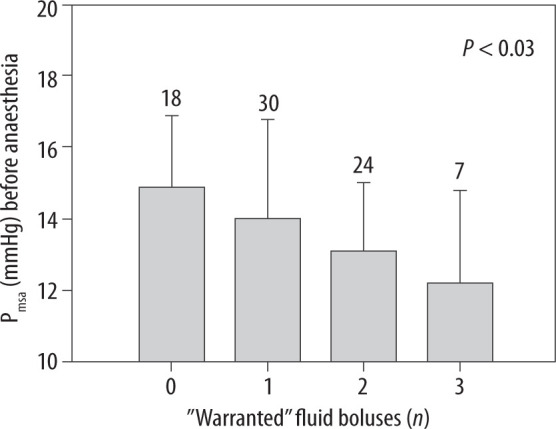
Pmsa was lower in fluid responders than in non-responders before induction (13.2 ± 2.2 vs. 14.7 ± 2.7 mmHg; mean ± SD, P < 0.01) and after induction of general anaesthesia (11.4 ± 2.1 vs. 12.8 ± 2.1 mmHg; P < 0.006). ROC curves showed that 14 mmHg before anaesthesia and 12 mmHg after anaesthesia induction served as optimal cut-offs for P msa to indicate fluid responsiveness. A linear correlation between P msa and blood volume changes suggested that the anaesthesia increased the unstressed blood volume by 1.2 L.
P msa was lower in fluid responders than in non-responders. General anaesthesia increased the need for blood volume by 1.2 L.
中心静脉压(Pms)均值在我们对循环的理解中起着核心作用。在一项临床试验的回顾性分析中,我们研究了 Pms 是否可以指示液体反应性,以及 Pms 是否可以指示麻醉诱导下非紧张血容量的增加,即不会增加跨壁压的容量。
在 86 名患者全麻诱导前和连续 3 次 3ml/kg 胶体液冲击后,基于心输出量、平均动脉压和中心静脉压计算出类似 Pms 的平均动脉压(Pmsa)。从冲击后液体量中增加的 ≥ 10%的每搏量表示液体反应性。使用接受者操作特征(ROC)曲线来寻找最佳 Pmsa 截断值以指示液体反应性。通过人体测量数据和血液稀释来估计血容量的变化。
在诱导前(13.2±2.2 比 14.7±2.7mmHg;均值±标准差,P<0.01)和全麻诱导后(11.4±2.1 比 12.8±2.1mmHg;P<0.006),液体反应者的 Pmsa 低于非反应者。ROC 曲线显示,麻醉前 14mmHg 和麻醉诱导后 12mmHg 是 Pmsa 指示液体反应性的最佳截断值。Pmsa 与血容量变化之间的线性相关性表明,麻醉增加了 1.2L 的非紧张血容量。
液体反应者的 Pmsa 低于非反应者。全麻增加了 1.2L 的血容量需求。