Division of Nephrology, Department of Medicine, Massachusetts General Hospital, Harvard Medical Center, Boston, Massachusetts.
Division of Nephrology, Department of Medicine, Western University, London, Ontario, Canada.
J Am Soc Nephrol. 2023 Apr 1;34(4):656-667. doi: 10.1681/ASN.0000000000000053. Epub 2023 Jan 30.
Pregnancies in women with CKD carry greater risk than pregnancies in the general population. The small number of women in prior studies has limited estimates of this risk, especially among those with advanced CKD. We report the results of a population-based cohort study in Ontario, Canada, that assessed more than 500,000 pregnancies, including 600 with a baseline eGFR < 60 ml/min per 1.73 m 2 . The investigation demonstrates increases in risk of different adverse maternal and fetal outcomes with lower eGFR and further risk elevation with baseline proteinuria.
CKD is a risk factor for pregnancy complications, but estimates for adverse outcomes come largely from single-center studies with few women with moderate or advanced stage CKD.
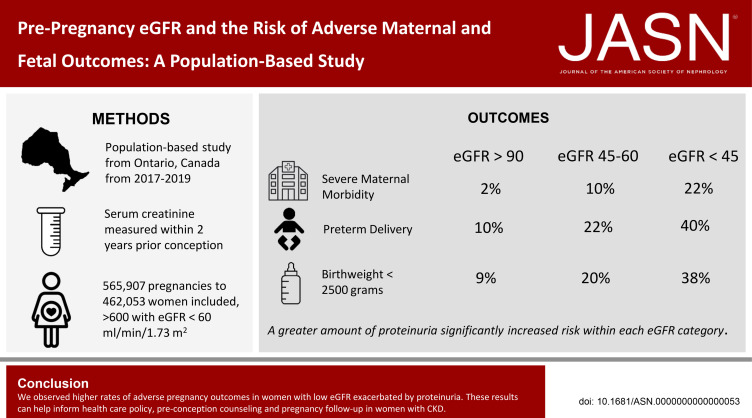
To investigate the association between maternal baseline eGFR and risk of adverse pregnancy outcomes, we conducted a retrospective, population-based cohort study of women (not on dialysis or having had a kidney transplant) in Ontario, Canada, who delivered between 2007 and 2019. The study included 565,907 pregnancies among 462,053 women. Administrative health databases captured hospital births, outpatient laboratory testing, and pregnancy complications. We analyzed pregnancies with serum creatinine measured within 2 years of conception up to 30 days after conception and assessed the impact of urine protein where available.
The risk of major maternal morbidity, preterm delivery, and low birthweight increased monotonically across declining eGFR categories, with risk increase most notable as eGFR dropped below 60 ml/min per 1.73 m 2 . A total of 56 (40%) of the 133 pregnancies with an eGFR <45 ml/min per 1.73 m 2 resulted in delivery under 37 weeks, compared with 10% of pregnancies when eGFR exceeded 90 ml/min per 1.73 m 2 . Greater proteinuria significantly increased risk within each eGFR category. Maternal and neonatal deaths were rare regardless of baseline eGFR (<0.3% of all pregnancies). Only 7% of women with an eGFR <45 ml/min per 1.73 m 2 received dialysis during or immediately after pregnancy.
We observed higher rates of adverse pregnancy outcomes in women with low eGFR with concurrent proteinuria. These results can help inform health care policy, preconception counseling, and pregnancy follow-up in women with CKD.
与普通人群相比,患有 CKD 的女性怀孕的风险更大。先前研究中的女性人数较少,这限制了对这种风险的估计,尤其是在那些患有晚期 CKD 的女性中。我们报告了一项在加拿大安大略省进行的基于人群的队列研究结果,该研究评估了超过 500,000 例妊娠,其中包括 600 例基线 eGFR < 60 ml/min/1.73 m 2 的妊娠。该研究表明,随着 eGFR 的降低和基线蛋白尿的进一步升高,不同不良母婴和胎儿结局的风险增加。
CKD 是妊娠并发症的一个危险因素,但不良结局的估计主要来自于少数女性的单中心研究,这些女性患有中重度 CKD。
为了研究母体基线 eGFR 与不良妊娠结局风险之间的关系,我们对加拿大安大略省的女性(未接受透析或肾移植)进行了一项回顾性、基于人群的队列研究,这些女性在 2007 年至 2019 年期间分娩。该研究包括 462,053 名女性的 565,907 例妊娠。行政健康数据库记录了医院分娩、门诊实验室检查和妊娠并发症。我们分析了在受孕后 2 年内测量血清肌酐值,直至受孕后 30 天的妊娠,并评估了尿液蛋白的影响。
主要产妇发病率、早产和低出生体重的风险随着 eGFR 类别逐渐下降而呈单调递增,当 eGFR 降至低于 60 ml/min/1.73 m 2 时,风险增加最为明显。共有 133 例 eGFR <45 ml/min/1.73 m 2 的妊娠中有 56 例(40%)分娩在 37 周以下,而 eGFR 超过 90 ml/min/1.73 m 2 的妊娠中仅 10%分娩在 37 周以下。在每个 eGFR 类别中,蛋白尿的大量增加显著增加了风险。无论基线 eGFR 如何(<所有妊娠的 0.3%),产妇和新生儿死亡都很少见。只有 7%的 eGFR <45 ml/min/1.73 m 2 的女性在怀孕期间或之后立即接受了透析。
我们观察到伴有蛋白尿的低 eGFR 女性的不良妊娠结局发生率更高。这些结果可以为 CKD 女性的医疗保健政策、孕前咨询和妊娠随访提供参考。