Department of Medicine, Division of Pulmonary Medicine, University of Alberta, Edmonton, AB, Canada.
Department of Medicine, Division of Respirology, University of Calgary, Calgary, AB, Canada.
BMJ. 2022 Dec 7;379:e071966. doi: 10.1136/bmj-2022-071966.
To determine the efficacy and safety of awake prone positioning versus usual care in non-intubated adults with hypoxemic respiratory failure due to covid-19.
Systematic review with frequentist and bayesian meta-analyses.
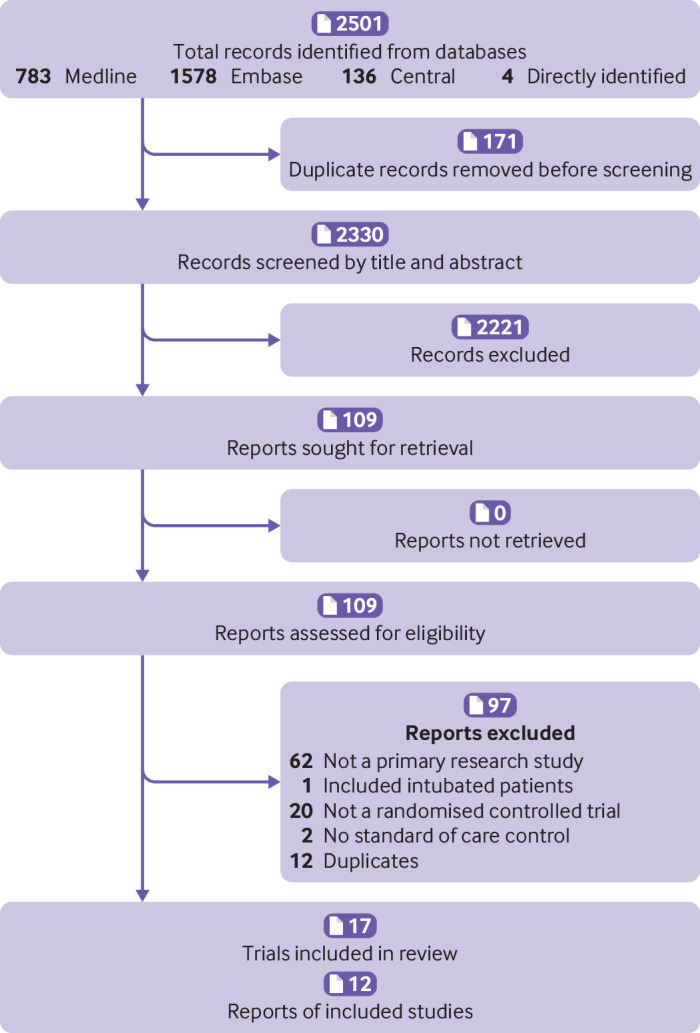
Randomized trials comparing awake prone positioning versus usual care in adults with covid-19 related hypoxemic respiratory failure. Information sources were Medline, Embase, and the Cochrane Central Register of Controlled Trials from inception to 4 March 2022.
Two reviewers independently extracted data and assessed risk of bias. Random effects meta-analyses were performed for the primary and secondary outcomes. Bayesian meta-analyses were performed for endotracheal intubation and mortality outcomes. GRADE certainty of evidence was assessed for outcomes.
The primary outcome was endotracheal intubation. Secondary outcomes were mortality, ventilator-free days, intensive care unit (ICU) and hospital length of stay, escalation of oxygen modality, change in oxygenation and respiratory rate, and adverse events.
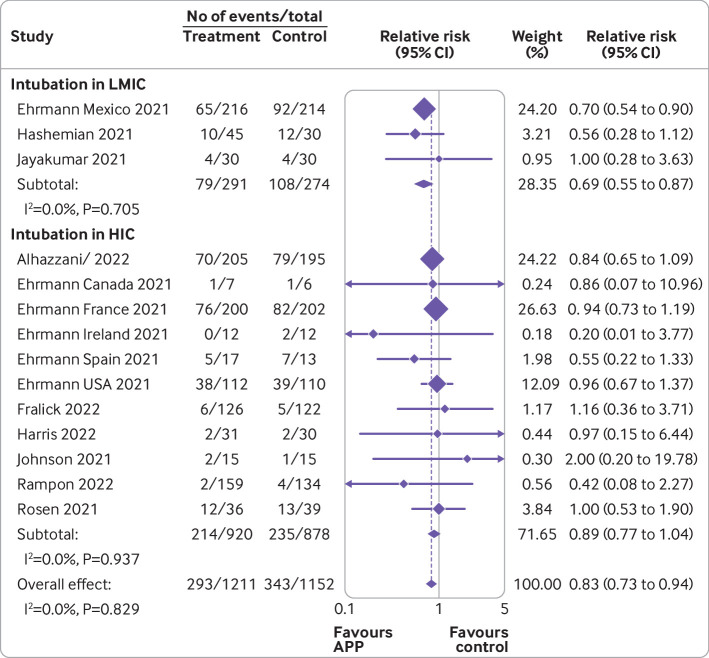
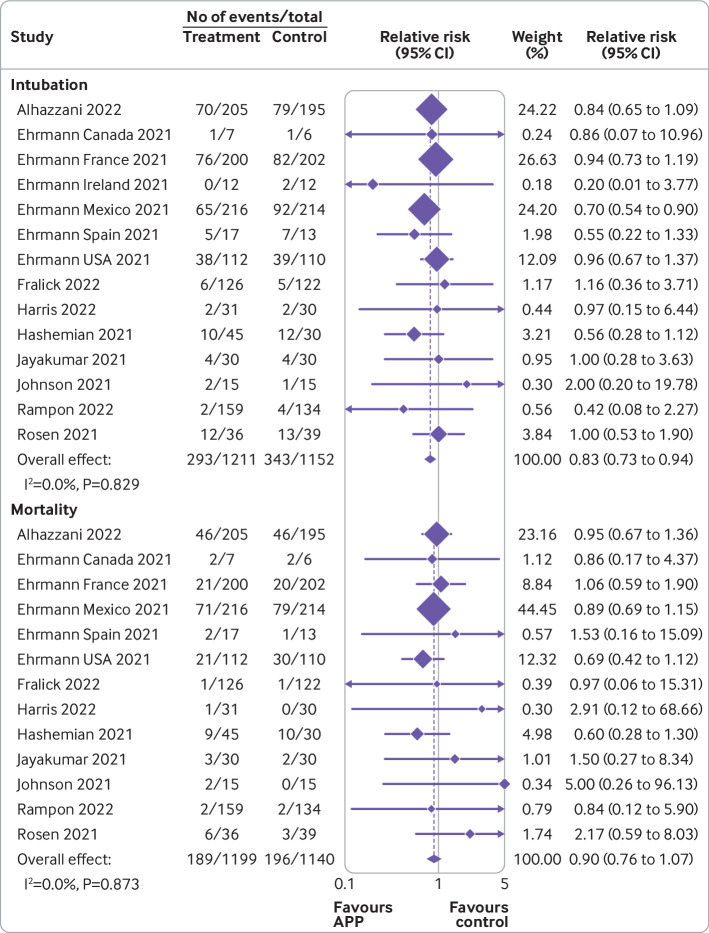
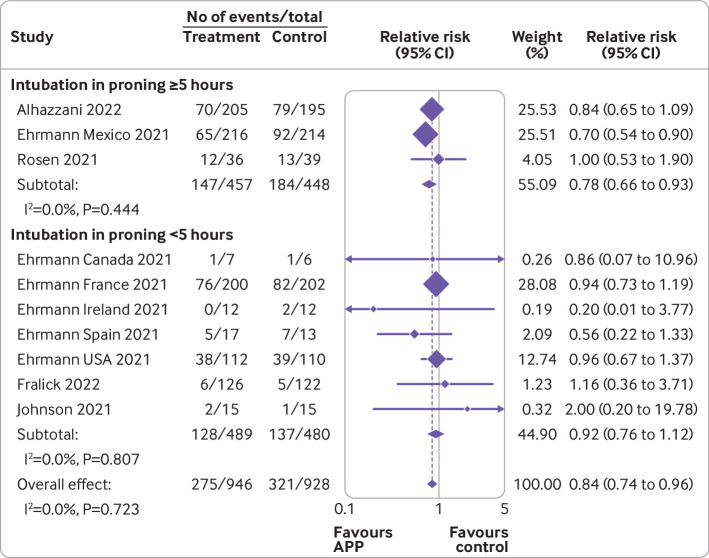
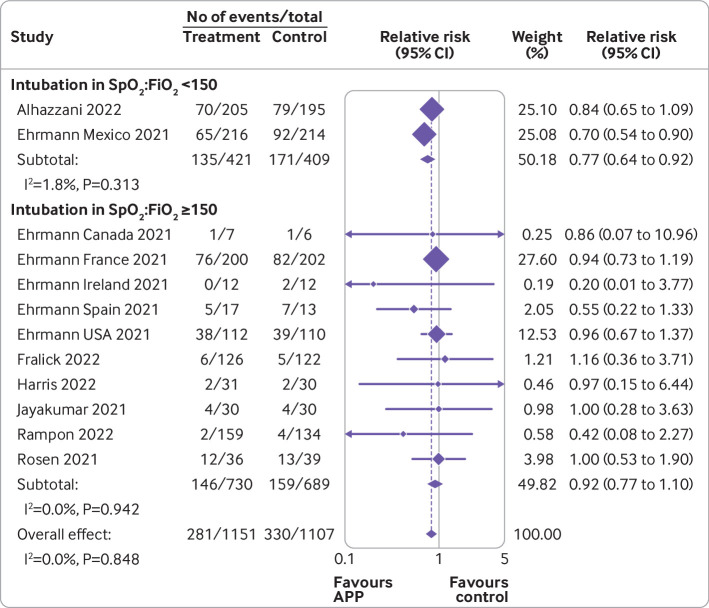
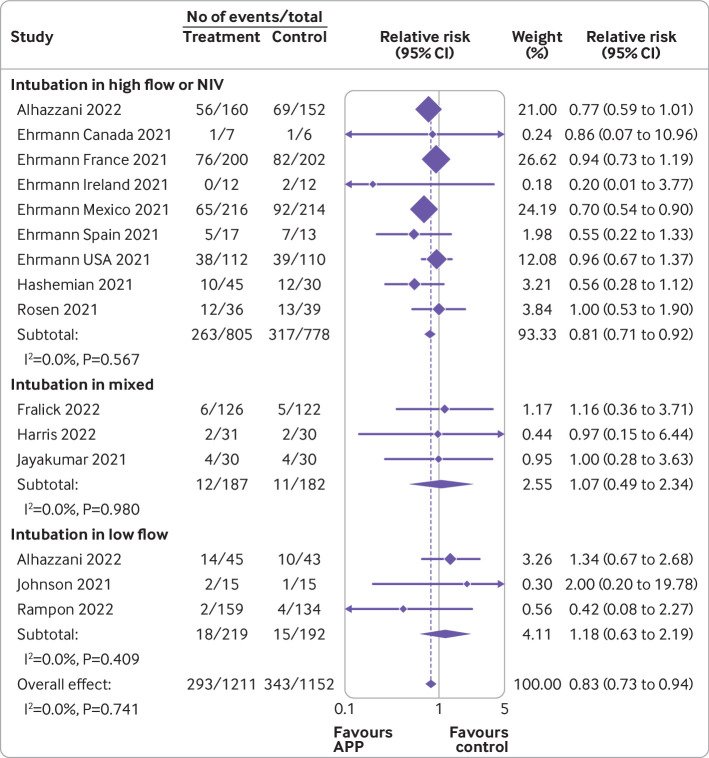
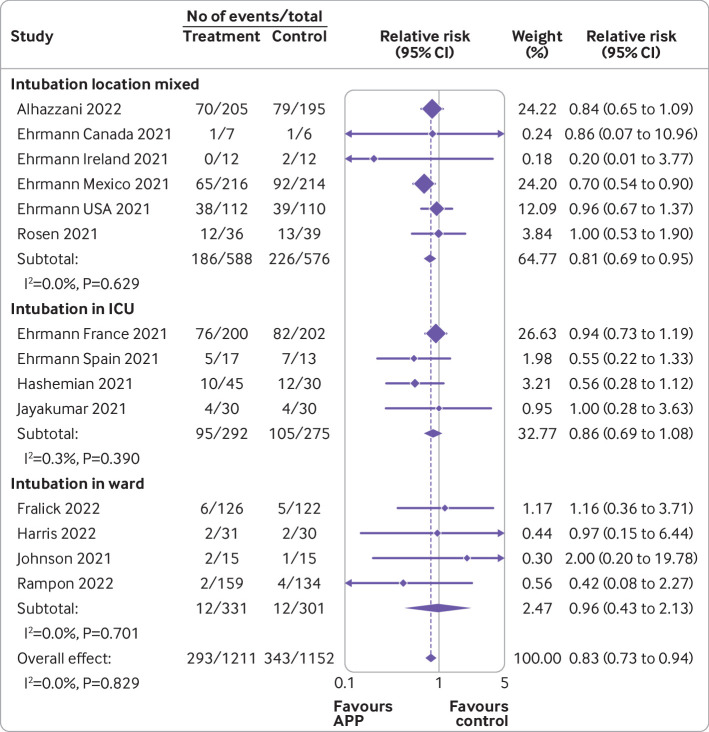
17 trials (2931 patients) met the eligibility criteria. 12 trials were at low risk of bias, three had some concerns, and two were at high risk. Awake prone positioning reduced the risk of endotracheal intubation compared with usual care (crude average 24.2% 29.8%, relative risk 0.83, 95% confidence interval 0.73 to 0.94; high certainty). This translates to 55 fewer intubations per 1000 patients (95% confidence interval 87 to 19 fewer intubations). Awake prone positioning did not significantly affect secondary outcomes, including mortality (15.6% 17.2%, relative risk 0.90, 0.76 to 1.07; high certainty), ventilator-free days (mean difference 0.97 days, 95% confidence interval -0.5 to 3.4; low certainty), ICU length of stay (-2.1 days, -4.5 to 0.4; low certainty), hospital length of stay (-0.09 days, -0.69 to 0.51; moderate certainty), and escalation of oxygen modality (21.4% 23.0%, relative risk 1.04, 0.74 to 1.44; low certainty). Adverse events related to awake prone positioning were uncommon. Bayesian meta-analysis showed a high probability of benefit with awake prone positioning for endotracheal intubation (non-informative prior, mean relative risk 0.83, 95% credible interval 0.70 to 0.97; posterior probability for relative risk <0.95=96%) but lower probability for mortality (0.90, 0.73 to 1.13; <0.95=68%).
Awake prone positioning compared with usual care reduces the risk of endotracheal intubation in adults with hypoxemic respiratory failure due to covid-19 but probably has little to no effect on mortality or other outcomes.
PROSPERO CRD42022314856.
评估清醒俯卧位与常规护理在新冠病毒导致的低氧性呼吸衰竭非插管成人患者中的疗效和安全性。
系统评价,包括频率论和贝叶斯荟萃分析。
比较清醒俯卧位与常规护理在新冠病毒相关低氧性呼吸衰竭成人患者中的随机试验。信息源为 Medline、Embase 和 Cochrane 对照试验中心注册库,从建库至 2022 年 3 月 4 日。
两位评审员独立提取数据并评估偏倚风险。主要和次要结局采用随机效应荟萃分析。贝叶斯荟萃分析用于气管插管和死亡率结局。采用 GRADE 评估证据确定性。
主要结局为气管插管。次要结局包括死亡率、无呼吸机天数、重症监护病房(ICU)和住院时间、氧疗方式升级、氧合和呼吸率变化以及不良事件。
17 项试验(2931 名患者)符合入选标准。12 项试验的偏倚风险较低,3 项存在一些顾虑,2 项风险较高。与常规护理相比,清醒俯卧位降低了气管插管的风险(粗平均 24.2% 29.8%,相对风险 0.83,95%置信区间 0.73 至 0.94;高确定性)。这意味着每 1000 名患者中可减少 55 例插管(95%置信区间 87 至 19 例减少)。清醒俯卧位并未显著影响次要结局,包括死亡率(15.6% 17.2%,相对风险 0.90,0.76 至 1.07;高确定性)、无呼吸机天数(平均差 0.97 天,95%置信区间 -0.5 至 3.4;低确定性)、ICU 住院时间(-2.1 天,-4.5 至 0.4;低确定性)、住院时间(-0.09 天,-0.69 至 0.51;中确定性)和氧疗方式升级(21.4% 23.0%,相对风险 1.04,0.74 至 1.44;低确定性)。与清醒俯卧位相关的不良事件并不常见。贝叶斯荟萃分析显示,清醒俯卧位在气管插管方面获益的可能性较高(无信息先验,平均相对风险 0.83,95%可信区间 0.70 至 0.97;后验相对风险<0.95 的概率=96%),但死亡率较低的可能性较小(0.90,0.73 至 1.13;<0.95 的概率=68%)。
与常规护理相比,清醒俯卧位可降低新冠病毒导致的低氧性呼吸衰竭非插管成人患者的气管插管风险,但可能对死亡率或其他结局几乎没有影响。
PROSPERO CRD42022314856。