Ding Cong, Jia Jianye, Han Lei, Zhou Wei, Liu Ziyan, Bai Genji, Wang Qian
Department of Radiology, The Affiliated Huaian No. 1 People's Hospital of Nanjing Medical University, Huaian, Jiangsu, China.
Department of Radiology, The Affiliated Huaian Hospital of Xuzhou Medical University, Huaian, Jiangsu, China.
Front Oncol. 2023 Jan 19;13:1036921. doi: 10.3389/fonc.2023.1036921. eCollection 2023.
Hepatectomy is the preferred treatment for patients with liver tumors. Post-hepatectomy liver failure (PHLF) remains one of the most fatal postoperative complications. We aim to explore the risk factors of PHLF and create a nomogram for early prediction of PHLF.
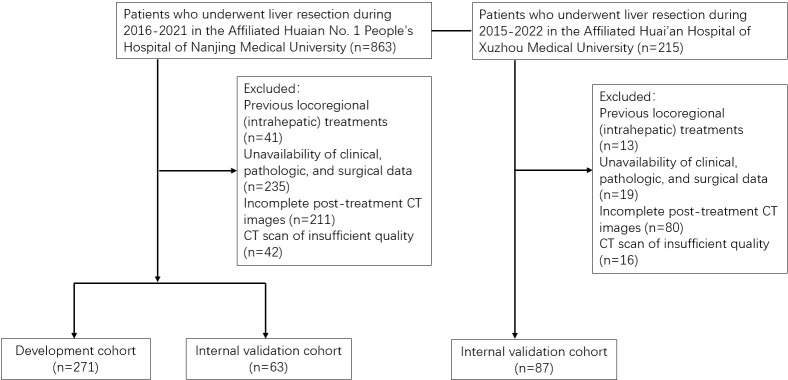
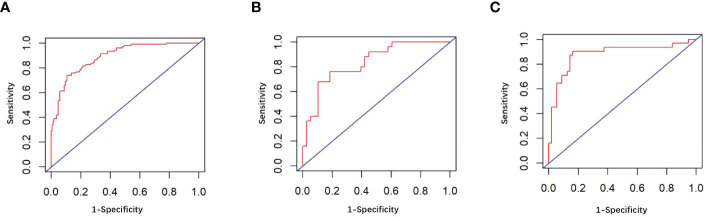
We retrospectively analyzed patients undergoing hepatectomy at the Affiliated Huaian No. 1 People's Hospital of Nanjing Medical University between 2015 and 2022, and the patients were divided into training and internal validation cohorts at an 8:2 ratio randomly. The patients undergoing liver resection from the Affiliated Huaian Hospital of Xuzhou Medical University worked as external validation. Then, a nomogram was developed which was based on multivariate analyses to calculate the risk of PHLF. The area under the ROC curve (AUROC) and Hosmer -Lemeshow test was used to evaluate the prediction effect of the model.
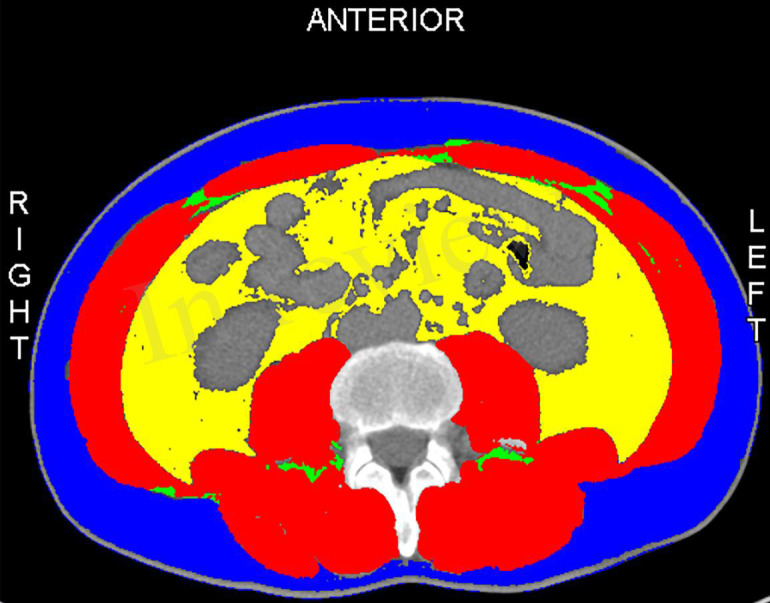
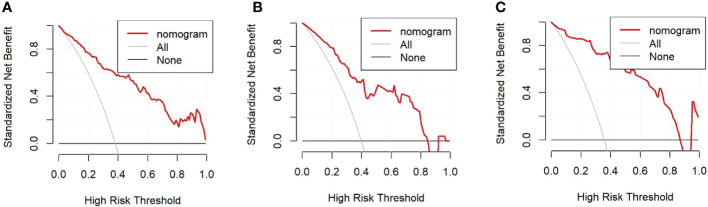
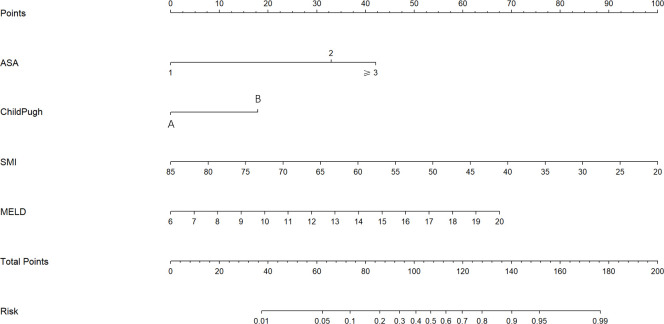
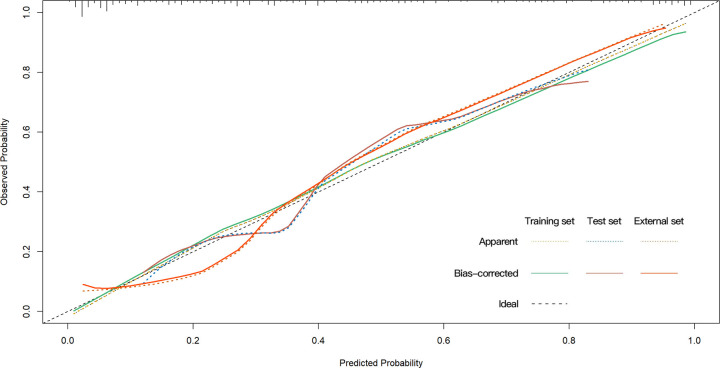
A total of 421 eligible patients were included in our study. Four preoperative variables were identified after multivariate analysis as follows, ASA (American Society of Anesthesiologists) score, Child-Pugh score, SMI (Skeletal muscle index), and MELD (Model for end-stage liver disease) score as independent predictors of PHLF. The area under the ROC curve of the predictive model in the training, internal, and external validation cohorts were 0.89, 0.82, and 0.89. Hosmer -Lemeshow P values in the training, internal, and external validation cohorts were 0.91, 0.22, and 0.15. The Calibration curve confirmed that our nomogram prediction results were in accurate agreement with the actual occurrence of PHLF.
We construct a nomogram to predict the grade B/C PHLF of ISGLS (International Study Group of Liver Surgery) in patients who underwent hepatic resection based on risk factors. This tool can provide a visual and accurate preoperative prediction of the grade B/C PHLF and guide the next step of clinical decision-making.
肝切除术是肝肿瘤患者的首选治疗方法。肝切除术后肝衰竭(PHLF)仍然是最致命的术后并发症之一。我们旨在探讨PHLF的危险因素,并创建一个列线图用于早期预测PHLF。
我们回顾性分析了2015年至2022年在南京医科大学附属淮安第一人民医院接受肝切除术的患者,并将患者以8:2的比例随机分为训练队列和内部验证队列。徐州医科大学附属淮安医院接受肝切除的患者作为外部验证。然后,基于多变量分析开发了一个列线图来计算PHLF的风险。采用ROC曲线下面积(AUROC)和Hosmer-Lemeshow检验来评估模型的预测效果。
我们的研究共纳入421例符合条件的患者。多变量分析后确定了四个术前变量,即美国麻醉医师协会(ASA)评分、Child-Pugh评分、骨骼肌指数(SMI)和终末期肝病模型(MELD)评分,作为PHLF的独立预测因素。预测模型在训练队列、内部验证队列和外部验证队列中的ROC曲线下面积分别为0.89、0.82和0.89。训练队列、内部验证队列和外部验证队列中的Hosmer-Lemeshow P值分别为0.91、0.22和0.15。校准曲线证实我们的列线图预测结果与PHLF的实际发生情况准确相符。
我们构建了一个列线图,用于根据危险因素预测接受肝切除患者的国际肝外科研究组(ISGLS)B/C级PHLF。该工具可以对B/C级PHLF进行直观准确的术前预测,并指导下一步的临床决策。