Department of Urology, Teikyo University Hospital, Mizonokuchi, 5-1-1, Futago, Takatsu-ku, Kawasaki City, Kanagawa Prefecture, 213-8507, Japan.
Department of Surgery, Teikyo University Hospital, Mizonokuchi, 5-1-1, Futago, Takatsu-ku, Kawasaki City, Kanagawa Prefecture, 213-8507, Japan.
World J Surg Oncol. 2023 Feb 6;21(1):37. doi: 10.1186/s12957-023-02920-2.
Renal cell carcinoma (RCC) and non-small cell lung cancer (NSCLC) are representative malignancies that respond well to immune checkpoint inhibitors (ICIs). Research has been conducted to identify biomarkers, such as programmed death ligand-1 (PD-L1), that would allow the response to ICI therapy to be predicted; however, the complex tumor immune system consisting of both host and tumor factors may also exert an influence.
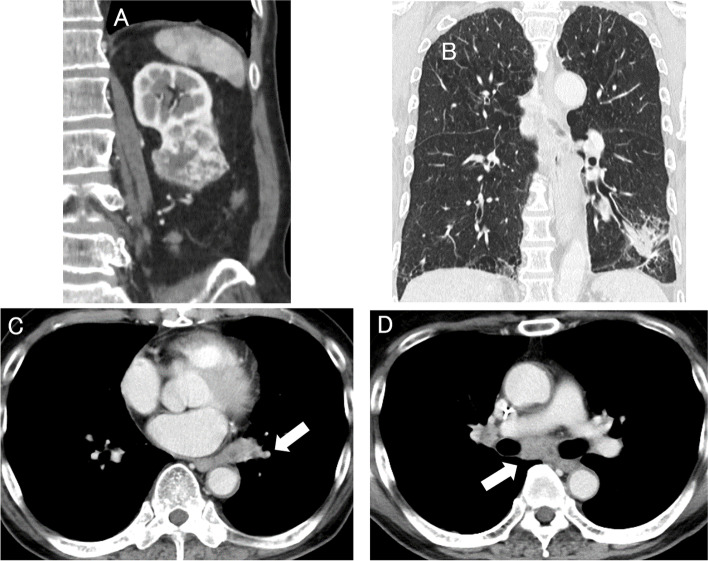
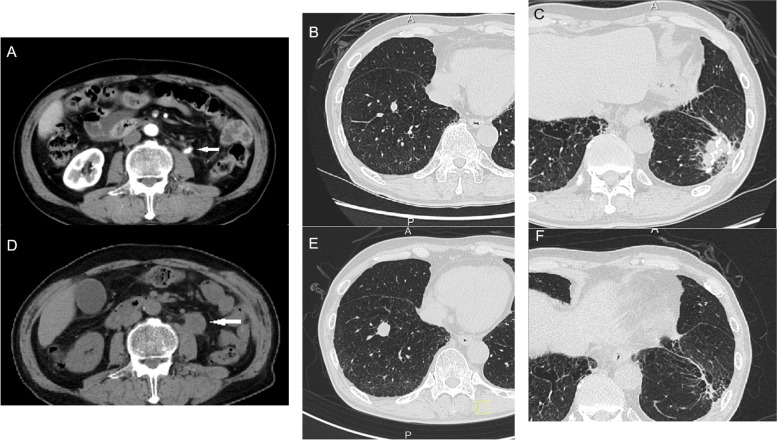
Computed tomographic imaging (CT) incidentally revealed a left renal mass, and a left pulmonary nodule with multiple lymph node metastases (LNMs). Firstly, video-assisted thoracic surgery revealed a lung tumor invading the chest wall. Histologically, the findings of the tumor were consistent with squamous cell carcinoma (SCC), and immunohistochemistry (IHC) showed positive PD-L1 expression. The renal tumor was excised by robotic-assisted partial nephrectomy (RAPN). Histologically, the renal tumor showed the features of clear cell carcinoma (CCC). Four months after the RAPN, CT revealed left hydronephrosis caused by an enhancing ureteral tumor. Then, multiple right lung metastases appeared, and the left lung tumor increased. Following treatment including atezolizumab, the primary lung SCC and the multiple LNMs almost disappeared completely, while the ureteral and right lung metastases showed progression. The ureteral metastasis was resected by left open nephroureterectomy. Histology of the ureteral tumor revealed features consistent with CCC. Histological examination of the multiple right lung metastases that were resected by partial lobectomy via a small thoracic incision also revealed features consistent with CCC. Two months after nephroureterectomy, a solitary left lung metastasis was treated by nivolumab and ipilimumab. Six months after nephroureterectomy, the patient died of RCC. Further studies of specimens revealed that the tumor cells in the primary RCC and the ureteral and lung metastases showed negative results of IHC for PD-L1.
The responses to ICI therapy of concomitant RCC and NSCLC were quite different. The PD-L1 expression status in individual tumors in cases of multiple primary malignancies (MPMs) may directly predict the response of each malignancy to ICI therapy, because the host immune system, which may affect the response to ICI therapy, could be the same in MPMs.
肾细胞癌(RCC)和非小细胞肺癌(NSCLC)是对免疫检查点抑制剂(ICI)反应良好的代表性恶性肿瘤。已经进行了研究以确定生物标志物,例如程序性死亡配体 1(PD-L1),从而可以预测对 ICI 治疗的反应;但是,由宿主和肿瘤因素组成的复杂肿瘤免疫系统也可能发挥作用。
计算机断层扫描(CT)偶然发现左肾肿块和多个肺门淋巴结转移(LNMs)的左肺结节。首先,电视辅助胸腔镜手术显示出侵犯胸壁的肺肿瘤。肿瘤的组织学检查结果与鳞状细胞癌(SCC)一致,免疫组织化学(IHC)显示 PD-L1 表达阳性。通过机器人辅助部分肾切除术(RAPN)切除肾肿瘤。组织学上,肾肿瘤表现出透明细胞癌(CCC)的特征。RAPN 后 4 个月,CT 显示左肾积水,由增强的输尿管肿瘤引起。然后,多个右肺转移灶出现,左肺肿瘤增大。阿特珠单抗治疗后,原发性肺 SCC 和多个 LNMs 几乎完全消失,而输尿管和右肺转移灶则显示进展。通过左开腹肾输尿管切除术切除输尿管转移灶。输尿管肿瘤的组织学检查结果与 CCC 一致。通过小切口部分肺叶切除术切除的多个右肺转移灶的组织学检查结果也与 CCC 一致。肾输尿管切除术后 2 个月,对单一左肺转移灶进行了纳武单抗和伊匹单抗治疗。肾输尿管切除术后 6 个月,患者死于 RCC。对标本的进一步研究表明,原发性 RCC、输尿管和肺部转移灶中的肿瘤细胞的 IHC 对 PD-L1 的检测结果均为阴性。
同时患有 RCC 和 NSCLC 的患者对 ICI 治疗的反应差异很大。在多原发恶性肿瘤(MPMs)中,个别肿瘤的 PD-L1 表达状态可能直接预测每种恶性肿瘤对 ICI 治疗的反应,因为可能影响 ICI 治疗反应的宿主免疫系统在 MPMs 中可能是相同的。