Cardio Center, IRCCS Humanitas Research Hospital, Rozzano, Milan, Italy.
Department of Biomedical Sciences, Humanitas University, Pieve Emanuele, Milan, Italy.
Cardiovasc Diabetol. 2023 Feb 6;22(1):28. doi: 10.1186/s12933-023-01744-4.
Despite paucity of data, it is common practice to discontinue metformin before invasive coronary angiography due to an alleged risk of Metformin-Associated Lactic Acidosis (M-ALA). We aimed at assessing the safety of metformin continuation in diabetic patients undergoing coronary angiography in terms of significant increase in lactate levels.
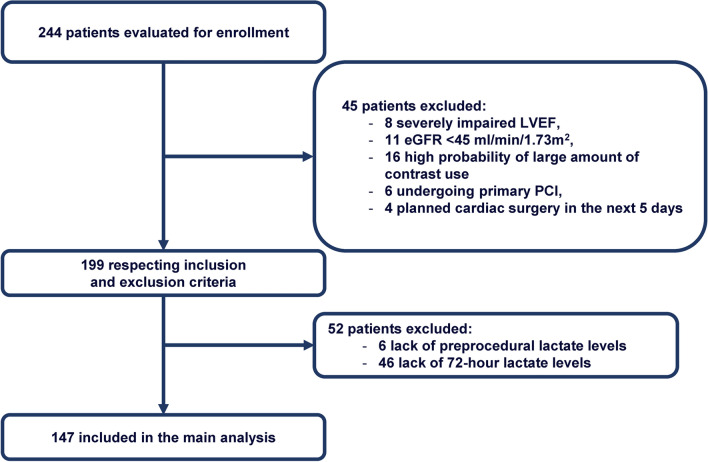
In this open-label, prospective, multicentre, single-arm trial, all diabetic patients undergoing coronary angiography with or without percutaneous coronary intervention at 3 European centers were screened for enrolment. The primary endpoint was the increase in lactate levels from preprocedural levels at 72-h after the procedure. Secondary endpoints included contrast associated-acute kidney injury (CA-AKI), M-ALA, and all-cause mortality.
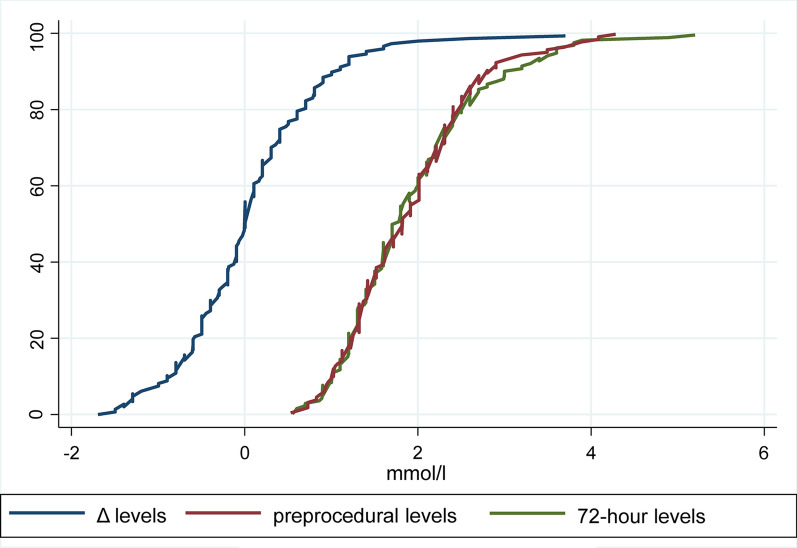
142 diabetic patients on metformin therapy were included. Median preprocedural lactate level was 1.8 mmol/l [interquartile range (IQR) 1.3-2.3]. Lactate levels at 72 h after coronary angiography were 1.7 mmol/l (IQR 1.3-2.3), with no significant differences as compared to preprocedural levels (p = 0.91; median difference = 0; IQR - 0.5 to 0.4 mmol/l). One patient had 72-h levels ≥ 5 mmol/l (5.3 mmol/l), but no cases of M-ALA were reported. CA-AKI occurred in 9 patients (6.1%) and median serum creatinine and estimated glomerular filtration rate remained similar throughout the periprocedural period. At a median follow-up of 90 days (43-150), no patients required hemodialysis and 2 patients died due to non-cardiac causes.
In diabetic patients undergoing invasive coronary angiography, metformin continuation throughout the periprocedural period does not increase lactate levels and was not associated with any decline in renal function.
The study was registered at Clinicaltrials.gov (NCT04766008).
尽管数据匮乏,但由于据称存在二甲双胍相关乳酸酸中毒(M-ALA)的风险,在进行有创冠状动脉造影检查前,通常会停用二甲双胍。我们旨在评估在接受冠状动脉造影检查的糖尿病患者中继续使用二甲双胍的安全性,其安全性通过检测血乳酸水平的显著升高来评估。
在这项开放标签、前瞻性、多中心、单臂试验中,在欧洲的 3 个中心筛选了所有接受冠状动脉造影术(伴或不伴经皮冠状动脉介入治疗)的糖尿病患者,以评估其入组情况。主要终点是在术后 72 小时内血乳酸水平从术前水平的升高。次要终点包括造影剂相关急性肾损伤(CA-AKI)、M-ALA 和全因死亡率。
共纳入 142 例接受二甲双胍治疗的糖尿病患者。术前乳酸中位数为 1.8mmol/L[四分位间距(IQR)1.3-2.3]。冠状动脉造影术后 72 小时的乳酸水平为 1.7mmol/L(IQR 1.3-2.3),与术前水平相比无显著差异(p=0.91;中位数差值=0;IQR -0.5 至 0.4mmol/L)。有 1 例患者 72 小时乳酸水平≥5mmol/L(5.3mmol/L),但未报告 M-ALA 病例。9 例(6.1%)患者发生 CA-AKI,整个围手术期血清肌酐和估算肾小球滤过率中位数保持相似。在中位 90 天(43-150)的随访中,无患者需要血液透析,2 例患者因非心脏原因死亡。
在接受有创冠状动脉造影检查的糖尿病患者中,整个围手术期继续使用二甲双胍不会增加乳酸水平,也不会导致肾功能下降。
该研究在 Clinicaltrials.gov 上注册(NCT04766008)。