Department of Pediatrics, Pediatric Transplant Hepatology, Miami Transplant Institute and University of Miami, Miami, Florida, USA.
Mirum Pharmaceuticals, Inc., Foster City, California, USA.
Liver Transpl. 2023 Jul 1;29(7):735-744. doi: 10.1097/LVT.0000000000000082. Epub 2023 Feb 8.
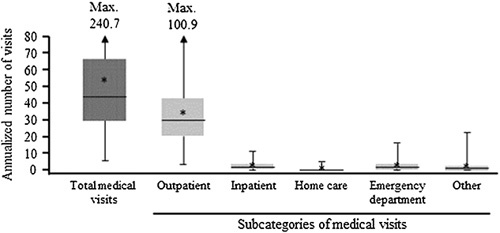
Children with rare cholestatic liver diseases, such as Alagille syndrome, progressive familial intrahepatic cholestasis, and biliary atresia typically require liver transplantation (LT). The objective of this analysis was to assess the economic burden of LT on these patients. Health care resource utilization and costs associated with pediatric LT were retrospectively assessed using insurance claims data from the US IBM MarketScan Commercial and Medicaid databases collected between October 2015 and December 2019. Inclusion criteria were as follows: ≥1 procedure code for LT, <18 years old at transplant, and ≥6 months of insurance eligibility at baseline. A cholestatic liver disease population who received LT was selected in the absence of specific diagnosis codes by excluding other severe liver conditions (ie, acute liver failure, malignancy) and by excluding severely decompensated individuals requiring ICU admission before LT. Annualized rates were reported. Over a mean study duration of 1.8 years, 53 commercially insured and 100 Medicaid-insured children received LT, with mean (SD) ages at baseline of 6.9 (6.0) and 5.7 (5.4) years, respectively. During this period, commercially insured and Medicaid-insured patients had annualized means of 65.3 and 52.8 medical visits, respectively. Most were outpatient visits, although the burden of inpatient visits was also high, with mean inpatient stays (inclusive of LT stay) of 37.2 and 31.6 days per year, respectively. Commercially insured and Medicaid-insured patients averaged US$512,124 and $211,863 in medical costs and $26,998 and $15,704 in pharmacy costs, respectively. These costs remained substantial throughout the first year after transplant. Overall, pediatric LT resulted in substantial health care resource utilization and cost burden in both commercially- and Medicaid-insured patients. Novel targeted medications that negate the need for pediatric LT could decrease the associated morbidity and costs.
患有罕见胆汁淤积性肝病(如 Alagille 综合征、进行性家族性肝内胆汁淤积症和胆道闭锁)的儿童通常需要进行肝移植(LT)。本分析旨在评估 LT 对这些患者的经济负担。使用美国 IBM MarketScan 商业和 Medicaid 数据库中 2015 年 10 月至 2019 年 12 月期间收集的保险索赔数据,回顾性评估与儿科 LT 相关的医疗资源利用和成本。纳入标准如下:至少有 1 次 LT 手术代码、移植时年龄<18 岁、基线时保险资格至少 6 个月。选择接受 LT 的胆汁淤积性肝病患者时,排除了其他严重肝脏疾病(如急性肝衰竭、恶性肿瘤)的特定诊断代码,并排除了 LT 前需要 ICU 入院治疗的严重失代偿个体,以此排除严重肝损伤患者。报告了年化率。在平均 1.8 年的研究期间,53 名商业保险和 100 名医疗补助保险的儿童接受了 LT,基线时的平均(SD)年龄分别为 6.9(6.0)和 5.7(5.4)岁。在此期间,商业保险和医疗补助保险患者的年化平均医疗就诊次数分别为 65.3 次和 52.8 次。大多数是门诊就诊,但住院就诊负担也很高,每年的平均住院天数(包括 LT 住院天数)分别为 37.2 天和 31.6 天。商业保险和医疗补助保险患者的医疗费用平均分别为 512124 美元和 211863 美元,药品费用分别为 26998 美元和 15704 美元。这些费用在移植后第一年仍然很高。总的来说,商业保险和医疗补助保险的患者接受儿科 LT 后,需要大量的医疗资源和费用。新型靶向药物可以避免儿科 LT,从而降低相关发病率和费用。