Shoffstall Andrew J, Gaebler Julia A, Kreher Nerissa C, Niecko Timothy, Douglas Diah, Strong Theresa V, Miller Jennifer L, Stafford Diane E, Butler Merlin G
Health Advances LLC, Weston, MA.
Health Advances LLC, Weston, MA.
J Pediatr. 2016 Aug;175:137-43. doi: 10.1016/j.jpeds.2016.05.018. Epub 2016 Jun 6.
To assess medical resource utilization associated with Prader-Willi syndrome (PWS) in the US, hypothesized to be greater relative to a matched control group without PWS.
We used a retrospective case-matched control design and longitudinal US administrative claims data (MarketScan) during a 5-year enrollment period (2009-2014). Patients with PWS were identified by Classification of Diseases, Ninth Revision, Clinical Modification diagnosis code 759.81. Controls were matched on age, sex, and payer type. Outcomes included total, outpatient, inpatient and prescription costs.
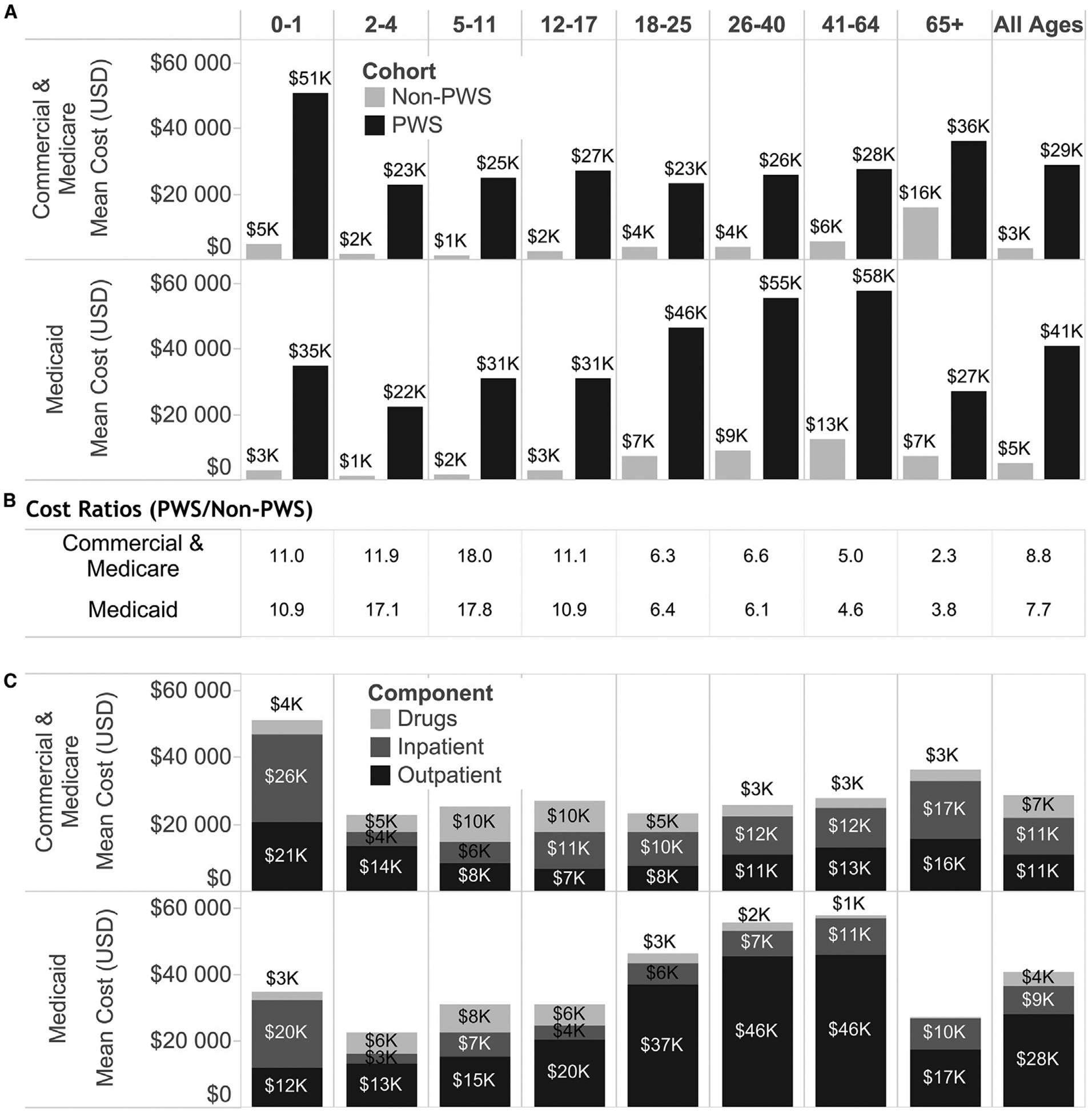
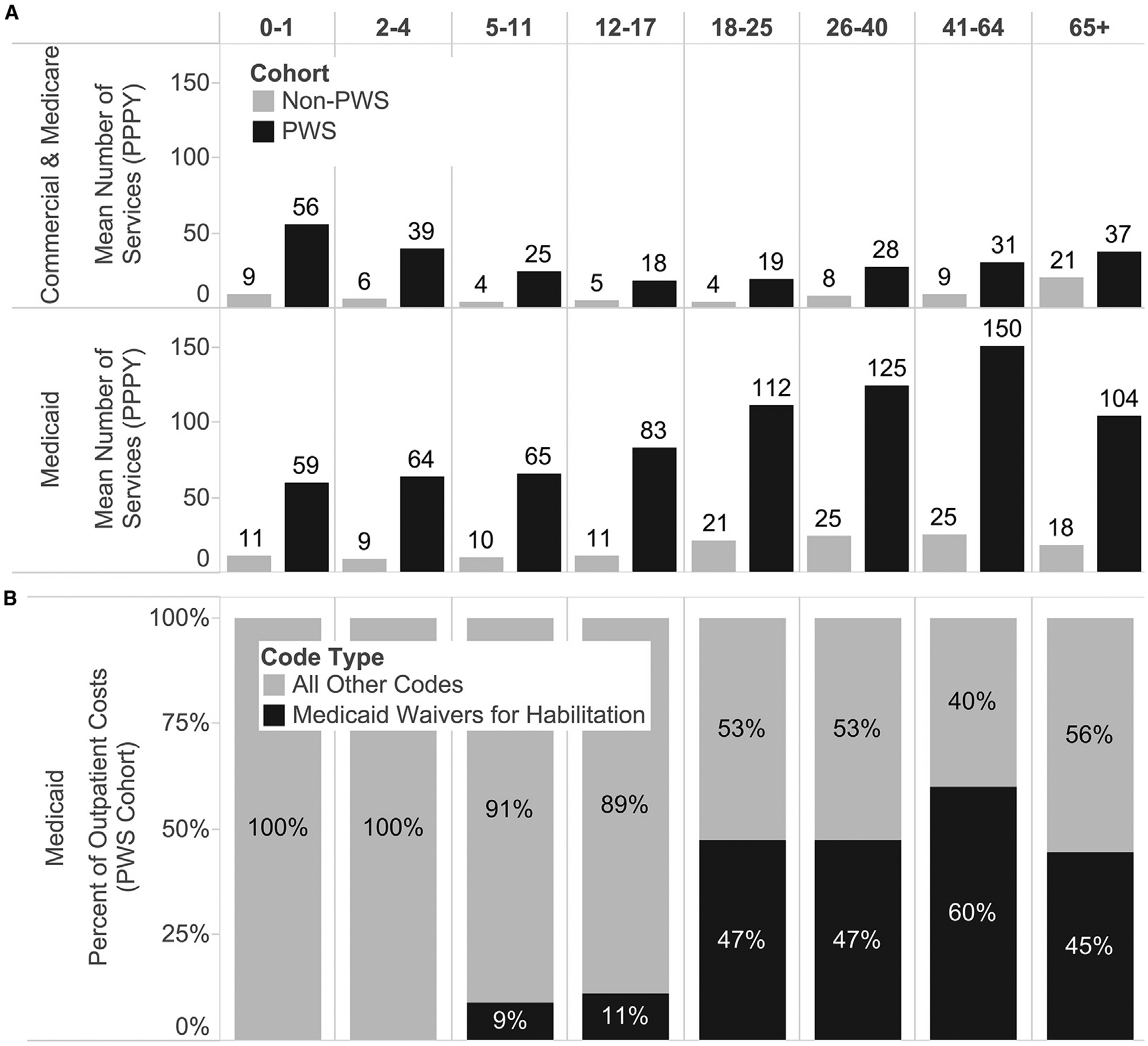
After matching and application of inclusion/exclusion criteria, we identified 2030 patients with PWS (1161 commercial, 38 Medicare supplemental, and 831 Medicaid). Commercially insured patients with PWS (median age 10 years) had 8.8-times greater total annual direct medical costs than their counterparts without PWS (median age 10 years: median costs $14 907 vs $819; P < .0001; mean costs: $28 712 vs $3246). Outpatient care comprised the largest portion of medical resource utilization for enrollees with and without PWS (median $5605 vs $675; P < .0001; mean $11 032 vs $1804), followed by mean annual inpatient and medication costs, which were $10 879 vs $1015 (P < .001) and $6801 vs $428 (P < .001), respectively. Total annual direct medical costs were ∼42% greater for Medicaid-insured patients with PWS than their commercially insured counterparts, an increase partly explained by claims for Medicaid Waiver day and residential habilitation.
Direct medical resource utilization was considerably greater among patients with PWS than members without the condition. This study provides a first step toward quantifying the financial burden of PWS posed to individuals, families, and society.
评估美国与普拉德-威利综合征(PWS)相关的医疗资源利用情况,假设其相对于无PWS的匹配对照组更高。
我们采用回顾性病例匹配对照设计,并利用美国在5年入组期(2009 - 2014年)的纵向行政索赔数据(MarketScan)。通过国际疾病分类第九版临床修订本诊断代码759.81识别出PWS患者。对照组在年龄、性别和付款人类型方面进行匹配。结果包括总费用、门诊费用、住院费用和处方费用。
在匹配并应用纳入/排除标准后,我们识别出2030例PWS患者(1161例商业保险患者、38例医疗保险补充患者和831例医疗补助患者)。商业保险的PWS患者(中位年龄10岁)每年的直接医疗总费用比无PWS的对应患者高8.8倍(中位年龄10岁:中位费用分别为14,907美元和819美元;P < 0.0001;平均费用分别为28,712美元和3246美元)。门诊护理在有和无PWS的参保者的医疗资源利用中占最大部分(中位费用分别为5605美元和675美元;P < 0.0001;平均费用分别为11,032美元和1804美元),其次是平均每年的住院和药物费用,分别为10,879美元和1015美元(P < 0.001)以及6801美元和428美元(P < 0.001)。医疗补助保险的PWS患者每年的直接医疗总费用比商业保险的对应患者高约42%,这一增长部分可由医疗补助豁免日和居家技能训练的索赔来解释。
PWS患者的直接医疗资源利用比无该疾病的成员显著更高。本研究为量化PWS给个人、家庭和社会带来的经济负担迈出了第一步。