Department of Family and Community Medicine, University of California, Davis, Sacramento.
Center for Healthcare Policy and Research, University of California, Davis, Sacramento.
JAMA Netw Open. 2023 Feb 1;6(2):e2255101. doi: 10.1001/jamanetworkopen.2022.55101.
Opioid tapering has been associated with negative consequences, such as increased overdoses and mental health needs. Tapering could also alter use of health care services and worsen care of comorbid conditions through disruption in primary care.
To evaluate tapering of stable long-term opioid therapy (LTOT) and subsequent health care service use and chronic condition care.
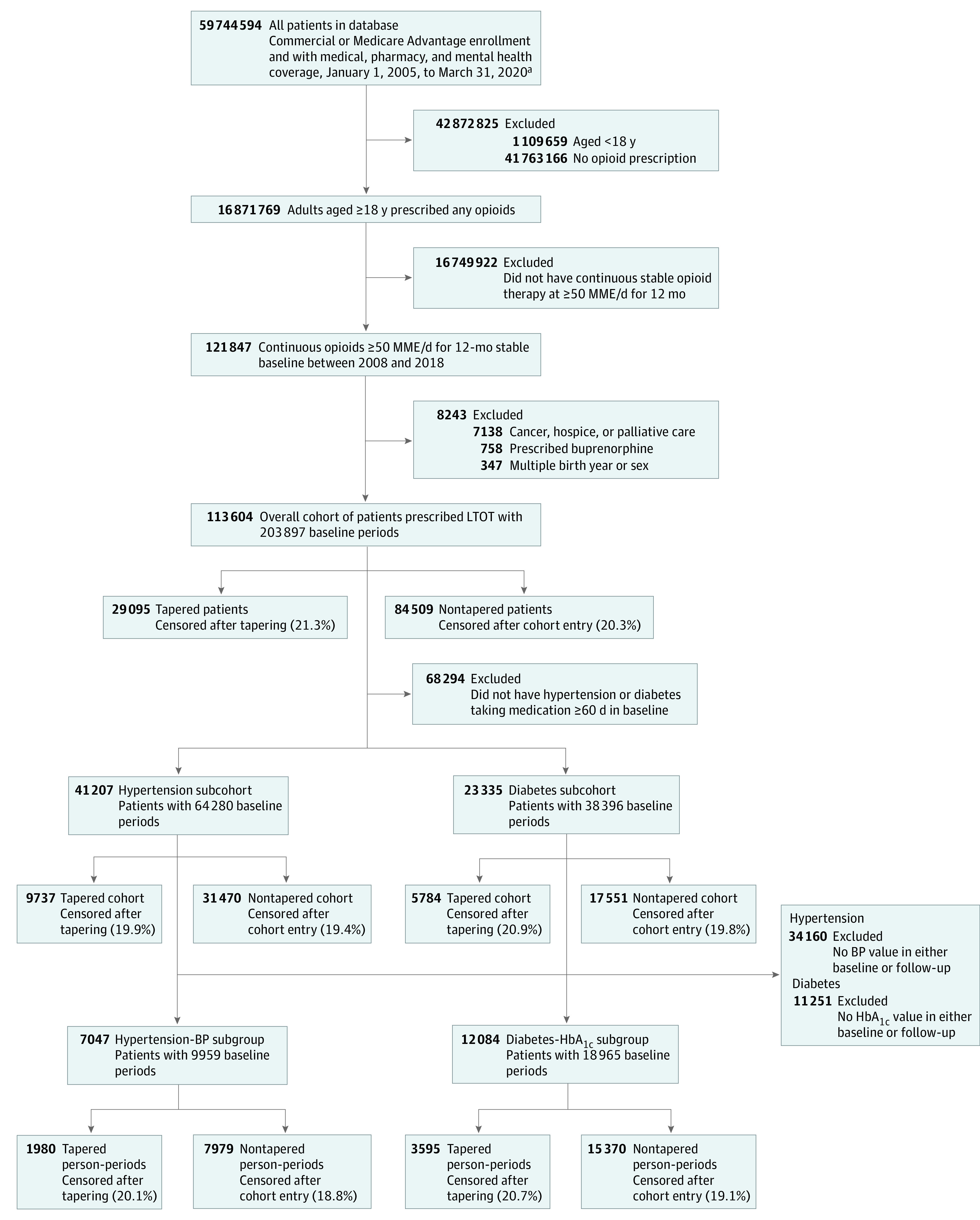
DESIGN, SETTING, AND PARTICIPANTS: A retrospective cohort study was conducted from January 1, 2008, to December 31, 2019. Data analysis was performed from July 9, 2020, to December 9, 2022. Data from the Optum Labs Data Warehouse, which contains deidentified retrospective administrative claims data and linked electronic health record data for commercial and Medicare Advantage enrollees, were used. Adults aged 18 years or older prescribed stable doses of LTOT at 50 morphine milligram equivalents or more per day during a 12-month baseline period were included, including subcohorts with hypertension or diabetes.
Opioid tapering, with 15% or more relative reduction in mean daily dose in 6 overlapping periods during 6 months.
Emergency department visits, hospitalizations, primary care and specialist visits, antihypertensive or antiglycemic medication adherence, and blood pressure and hemoglobin A1c levels during up to 12 months' follow-up. Covariates included sociodemographic characteristics, comorbidities, health care use, and chronic condition control.
Among 113 604 patients (60 764 [53.5%] women; mean [SD] age, 58.1 [11.8] years) prescribed LTOT, 41 207 had hypertension and 23 335 had diabetes; in all cohorts, approximately half were women, and half were aged 50 to 65 years. In the overall cohort, tapering was associated with more emergency department visits (adjusted incidence rate ratio [aIRR], 1.19; 95% CI, 1.16-1.21) and hospitalizations (aIRR, 1.16; 95% CI, 1.12-1.20), with similar magnitude associations in the hypertension and diabetes subcohorts. Tapering was associated with fewer primary care visits in the overall cohort (aIRR, 0.95; 95% CI, 0.94-0.96) and hypertension subcohort (aIRR, 0.98; 95% CI, 0.97-0.99). For the hypertension or diabetes subcohorts, tapering was associated with reduced medication adherence (hypertension: aIRR, 0.60; 95% CI, 0.59-0.62; diabetes: aIRR, 0.69; 95% CI, 0.67-0.71) and small increases in diastolic blood pressure and hemoglobin A1c level.
In this cohort study of patients prescribed LTOT, opioid tapering was associated with more emergency department visits and hospitalizations, fewer primary care visits, and reduced antihypertensive and antidiabetic medication adherence. These outcomes may represent unintended negative consequences of opioid tapering for policy makers and clinicians to consider.
阿片类药物的逐渐减少与一些负面后果有关,例如增加过量用药和心理健康需求。逐渐减少也可能通过破坏初级保健来改变卫生保健服务的使用情况,并恶化合并症的护理。
评估稳定的长期阿片类药物治疗 (LTOT) 的逐渐减少以及随后的卫生保健服务使用情况和慢性疾病护理情况。
设计、设置和参与者:这是一项从 2008 年 1 月 1 日至 2019 年 12 月 31 日进行的回顾性队列研究。数据分析于 2020 年 7 月 9 日至 2022 年 12 月 9 日进行。使用了来自 Optum Labs 数据仓库的数据,该数据库包含了商业和医疗保险优势计划参与者的匿名回顾性行政索赔数据和相关的电子健康记录数据。纳入了在 12 个月基线期内每天服用稳定剂量 LTOT(50 毫克吗啡当量或以上)的年龄在 18 岁或以上的成年人,包括患有高血压或糖尿病的亚组。
在 6 个月的 6 个重叠期间,每日平均剂量减少 15%或更多。
在长达 12 个月的随访期间,急诊就诊、住院、初级保健和专科就诊、降压或降糖药物的依从性,以及血压和糖化血红蛋白水平。协变量包括社会人口统计学特征、合并症、卫生保健使用情况和慢性疾病控制情况。
在 113604 名接受 LTOT 治疗的患者(60764[53.5%]名女性;平均[标准差]年龄,58.1[11.8]岁)中,41207 名患有高血压,23335 名患有糖尿病;在所有队列中,大约一半是女性,一半年龄在 50 岁至 65 岁之间。在总体队列中,逐渐减少与更多的急诊就诊(调整后的发病率比[aIRR],1.19;95%置信区间[CI],1.16-1.21)和住院(aIRR,1.16;95%CI,1.12-1.20)有关,在高血压和糖尿病亚组中也有类似的关联。逐渐减少与总体队列(aIRR,0.95;95%CI,0.94-0.96)和高血压亚组(aIRR,0.98;95%CI,0.97-0.99)的初级保健就诊次数减少有关。对于高血压或糖尿病亚组,逐渐减少与药物依从性降低有关(高血压:aIRR,0.60;95%CI,0.59-0.62;糖尿病:aIRR,0.69;95%CI,0.67-0.71),舒张压和糖化血红蛋白水平略有升高。
在这项接受 LTOT 治疗的患者队列研究中,阿片类药物的逐渐减少与更多的急诊就诊和住院、更少的初级保健就诊以及降压和降糖药物的依从性降低有关。这些结果可能是政策制定者和临床医生需要考虑的阿片类药物逐渐减少的意外负面后果。