Veterans Affairs Program Evaluation and Resource Center, Veterans Affairs Office of Mental Health and Suicide Prevention, Menlo Park, CA, USA
Veterans Affairs Center for Innovation to Implementation, Veterans Affairs Palo Alto Health Care System, 795 Willow Road, Building 324, Menlo Park, CA 94025, USA.
BMJ. 2020 Mar 4;368:m283. doi: 10.1136/bmj.m283.
To examine the associations between stopping treatment with opioids, length of treatment, and death from overdose or suicide in the Veterans Health Administration.
Observational evaluation.
Veterans Health Administration.
1 394 102 patients in the Veterans Health Administration with an outpatient prescription for an opioid analgesic from fiscal year 2013 to the end of fiscal year 2014 (1 October 2012 to 30 September 2014).
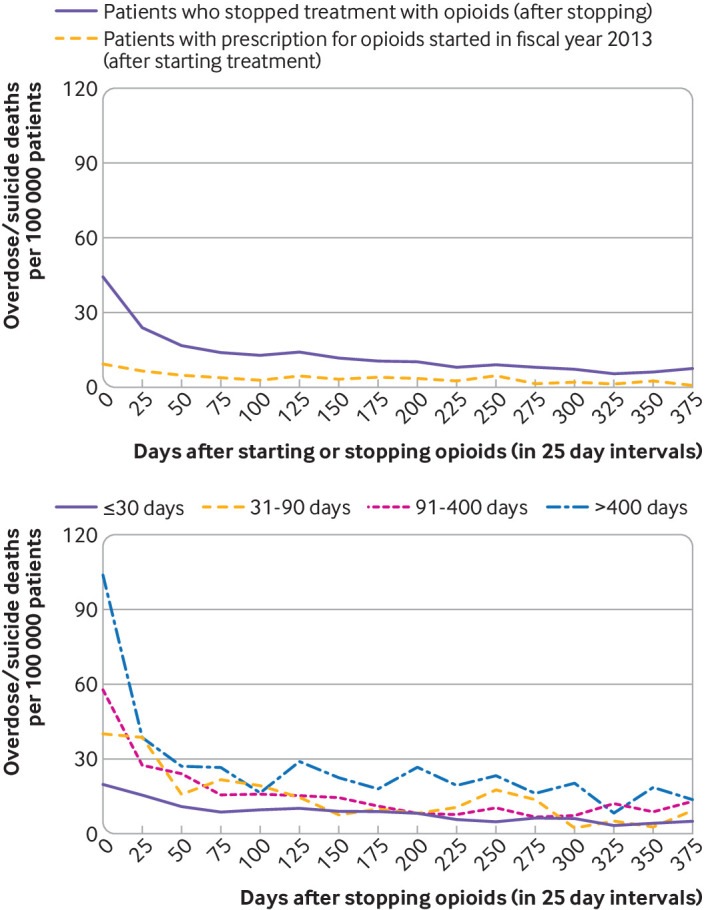
A multivariable Cox non-proportional hazards regression model examined death from overdose or suicide, with the interaction of time varying opioid cessation by length of treatment (≤30, 31-90, 91-400, and >400 days) as the main covariates. Stopping treatment with opioids was measured as the time when a patient was estimated to have no prescription for opioids, up to the end of the next fiscal year (2014) or the patient's death.
2887 deaths from overdose or suicide were found. The incidence of stopping opioid treatment was 57.4% (n799 668) overall, and based on length of opioid treatment was 32.0% (≤30 days), 8.7% (31-90 days), 22.7% (91-400 days), and 36.6% (>400 days). The interaction between stopping treatment with opioids and length of treatment was significant (P<0.001); stopping treatment was associated with an increased risk of death from overdose or suicide regardless of the length of treatment, with the risk increasing the longer patients were treated. Hazard ratios for patients who stopped opioid treatment (with reference values for all other covariates) were 1.67 (≤30 days), 2.80 (31-90 days), 3.95 (91-400 days), and 6.77 (>400 days). Descriptive life table data suggested that death rates for overdose or suicide increased immediately after starting or stopping treatment with opioids, with the incidence decreasing over about three to 12 months.
Patients were at greater risk of death from overdose or suicide after stopping opioid treatment, with an increase in the risk the longer patients had been treated before stopping. Descriptive data suggested that starting treatment with opioids was also a risk period. Strategies to mitigate the risk in these periods are not currently a focus of guidelines for long term use of opioids. The associations observed cannot be assumed to be causal; the context in which opioid prescriptions were started and stopped might contribute to risk and was not investigated. Safer prescribing of opioids should take a broader view on patient safety and mitigate the risk from the patient's perspective. Factors to address are those that place patients at risk for overdose or suicide after beginning and stopping opioid treatment, especially in the first three months.
在退伍军人健康管理局(Veterans Health Administration,VHA)中,研究停止使用阿片类药物治疗、治疗时间长短与因药物过量或自杀导致的死亡之间的关联。
观察性评估。
退伍军人健康管理局。
2013 财年至 2014 财年末(2012 年 10 月 1 日至 2014 年 9 月 30 日)期间,VHA 门诊开处阿片类镇痛药处方的 1394102 例患者。
多变量 Cox 非比例风险回归模型检查了因药物过量或自杀导致的死亡情况,主要协变量是治疗时间长短(≤30、31-90、91-400 和>400 天)与时间变化的阿片类药物停药的相互作用。停止使用阿片类药物的治疗时间定义为患者估计没有阿片类药物处方的时间,直至下一个财政年度(2014 年)结束或患者死亡。
共发现 2887 例因药物过量或自杀导致的死亡。总体上,停止阿片类药物治疗的发生率为 57.4%(n=799668),根据阿片类药物治疗时间长短,分别为 32.0%(≤30 天)、8.7%(31-90 天)、22.7%(91-400 天)和 36.6%(>400 天)。阿片类药物停药与治疗时间之间的交互作用具有统计学意义(P<0.001);无论治疗时间长短如何,停止治疗都会增加药物过量或自杀导致的死亡风险,且随着患者治疗时间的延长,风险会增加。与所有其他协变量相比,停止阿片类药物治疗的患者的危险比为 1.67(≤30 天)、2.80(31-90 天)、3.95(91-400 天)和 6.77(>400 天)。描述性生存表数据表明,在开始或停止使用阿片类药物治疗后,药物过量或自杀的死亡率立即上升,约 3 至 12 个月后下降。
停止阿片类药物治疗后,患者因药物过量或自杀导致死亡的风险更高,且在停止治疗前治疗时间越长,风险越大。描述性数据表明,开始使用阿片类药物也是一个风险期。目前,长期使用阿片类药物指南并未将减少这些时期风险的策略作为重点。观察到的关联不能被假定为因果关系;阿片类药物处方开始和停止的背景可能会增加风险,而这一点尚未得到调查。安全开具阿片类药物应从更广泛的患者安全角度出发,并从患者的角度减轻风险。需要解决的因素是那些使患者在开始和停止阿片类药物治疗后有药物过量或自杀风险的因素,尤其是在头三个月。