Department of Head and Neck Surgery; Houston, Texas, USA.
Endocrine Neoplasia and Hormonal Disorders; Houston, Texas, USA.
Thyroid. 2023 Apr;33(4):484-491. doi: 10.1089/thy.2022.0504. Epub 2023 Mar 20.
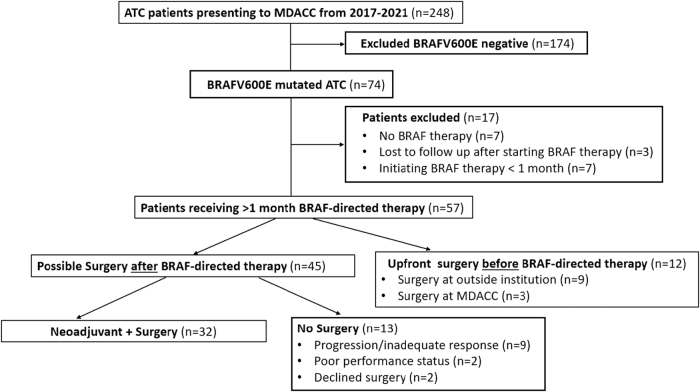
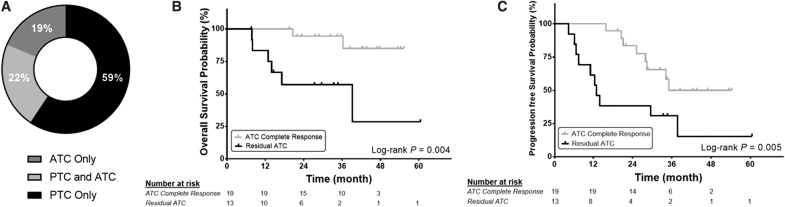
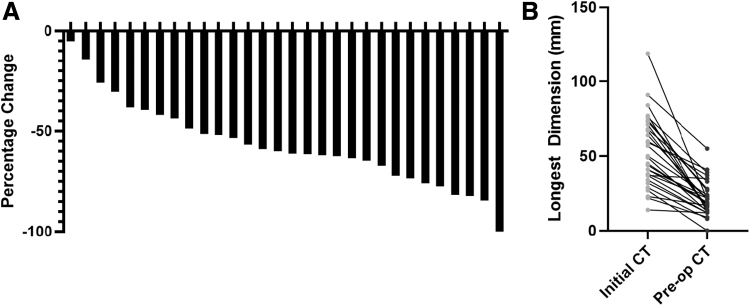
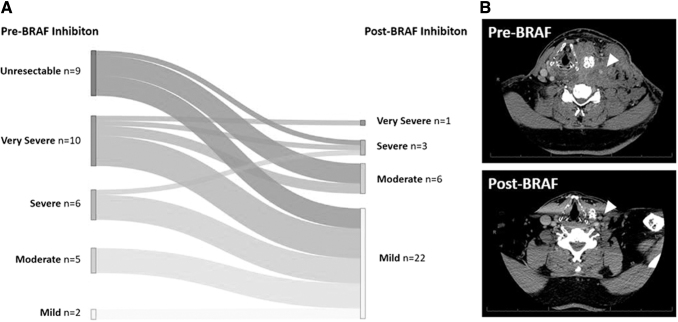
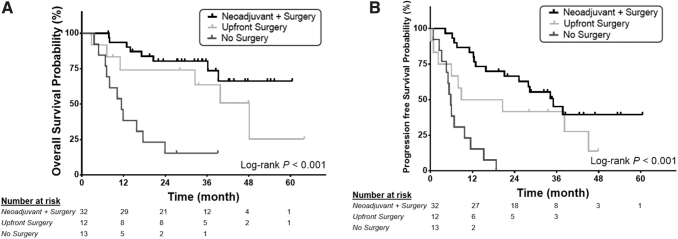
The aim of this study was to describe the oncologic outcomes of patients with BRAF-mutated anaplastic thyroid cancer (ATC) who had neoadjuvant BRAF-directed therapy with subsequent surgery. For context, we also reviewed patients who received BRAF-directed therapy after surgery, and those who did not have surgery after BRAF-directed therapy. This was a single-center retrospective cohort study conducted at a tertiary care cancer center in Texas from 2017 to 2021. Fifty-seven consecutive patients with BRAF-mutated ATC and at least 1 month of BRAF-directed therapy were included. Primary outcomes were overall survival (OS) and progression-free survival (PFS). All patients had stage IVB (35%) or IVC (65%) ATC. Approximately 70% of patients treated with BRAF-directed therapy ultimately had surgical resection of residual disease. Patients who had neoadjuvant BRAF-directed therapy followed by surgery ( = 32) had 12-month OS of 93.6% [confidence interval (CI) 84.9-100] and PFS of 84.4% [CI 71.8-96.7]. Patients who had surgery before BRAF-directed therapy ( = 12) had 12-month OS of 74.1% [CI 48.7-99.5] and PFS of 50% [CI 21.7-78.3]. Finally, patients who did not receive surgery after BRAF-directed therapy ( = 13) had 12-month OS of 38.5% [CI 12.1-64.9] and PFS of 15.4% [CI 0-35.0]. Neoadjuvant BRAF-directed therapy reduced tumor size, extent of surgery, and surgical morbidity score. Subgroup analysis suggested that any residual ATC in the surgical specimen was associated with significantly worse 12-month OS and PFS (OS = 83.3% [CI 62.6-100], PFS = 61.5% [CI 35.1-88]) compared with patients with pathologic ATC complete response (OS = 100%, PFS = 100%). We observed that neoadjuvant BRAF-directed therapy reduced extent of surgery and surgical morbidity. While acknowledging potential selection bias, the 12-month OS rate appeared higher in patients who had BRAF-directed therapy followed by surgery as compared with BRAF-directed therapy without surgery; yet, it was not significantly different from surgery followed by BRAF-directed therapy. PFS appeared higher in patients treated with neoadjuvant BRAF-directed therapy relative to patients in the other groups. These promising results of neoadjuvant BRAF-directed therapy followed by surgery for BRAF-mutated ATC should be confirmed in prospective clinical trials.
这项研究的目的是描述接受新辅助 BRAF 靶向治疗后接受手术的 BRAF 突变型间变性甲状腺癌(ATC)患者的肿瘤学结局。为此,我们还回顾了接受手术后 BRAF 靶向治疗的患者,以及未接受 BRAF 靶向治疗后手术的患者。这是一项单中心回顾性队列研究,在德克萨斯州的一家三级癌症中心进行,时间为 2017 年至 2021 年。共纳入 57 例 BRAF 突变型 ATC 且至少接受 1 个月 BRAF 靶向治疗的连续患者。主要结局为总生存期(OS)和无进展生存期(PFS)。所有患者均为 IVB 期(35%)或 IVC 期(65%)ATC。约 70%的接受 BRAF 靶向治疗的患者最终接受了残留疾病的手术切除。接受新辅助 BRAF 靶向治疗后手术( = 32)的患者 12 个月 OS 率为 93.6%[置信区间(CI)84.9-100],PFS 率为 84.4%[CI 71.8-96.7]。接受 BRAF 靶向治疗前手术( = 12)的患者 12 个月 OS 率为 74.1%[CI 48.7-99.5],PFS 率为 50%[CI 21.7-78.3]。最后,接受 BRAF 靶向治疗后未手术的患者( = 13)12 个月 OS 率为 38.5%[CI 12.1-64.9],PFS 率为 15.4%[CI 0-35.0]。新辅助 BRAF 靶向治疗可缩小肿瘤大小、手术范围和手术发病率评分。亚组分析表明,手术标本中任何残留的 ATC 与 12 个月 OS 和 PFS 显著更差相关(OS = 83.3%[CI 62.6-100],PFS = 61.5%[CI 35.1-88]),与病理 ATC 完全缓解的患者相比(OS = 100%,PFS = 100%)。我们观察到新辅助 BRAF 靶向治疗可减少手术范围和手术发病率。虽然承认存在潜在的选择偏倚,但与未接受 BRAF 靶向治疗的患者相比,接受 BRAF 靶向治疗后手术的患者 12 个月 OS 率似乎更高;然而,与接受 BRAF 靶向治疗后手术的患者相比,这并没有显著差异。与其他组相比,接受新辅助 BRAF 靶向治疗的患者 PFS 更高。对于 BRAF 突变型 ATC,新辅助 BRAF 靶向治疗后手术的这些有希望的结果应在前瞻性临床试验中得到证实。