Danish Headache Center, Department of Neurology, Rigshospitalet - Glostrup, Faculty of Health and Medical Sciences, University of Copenhagen, Valdemar Hansen Vej 5, 2600, Glostrup, Denmark.
Danish Headache Knowledge Center, Rigshospitalet - Glostrup, Glostrup, Denmark.
Neurotherapeutics. 2023 Mar;20(2):389-398. doi: 10.1007/s13311-023-01350-y. Epub 2023 Feb 10.
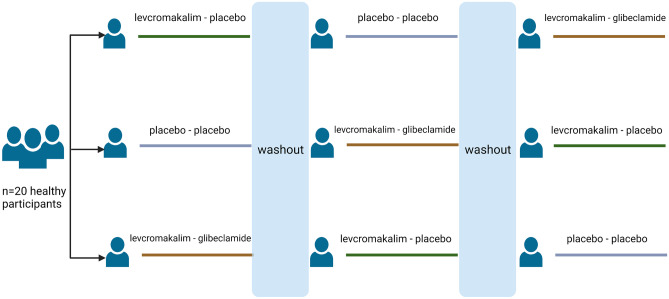
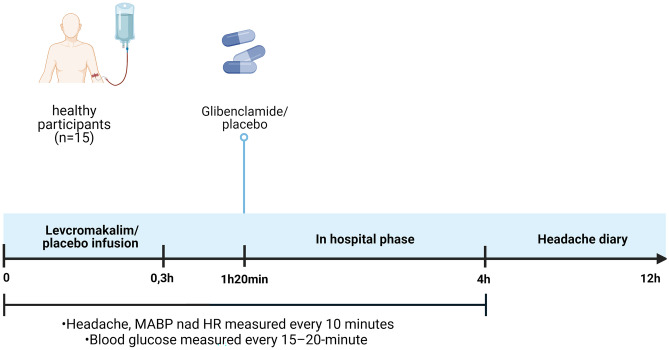
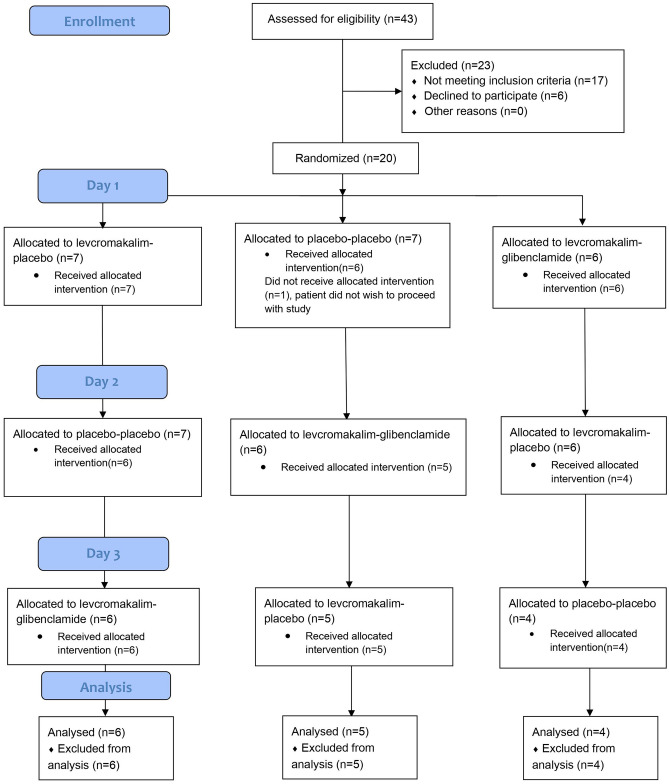
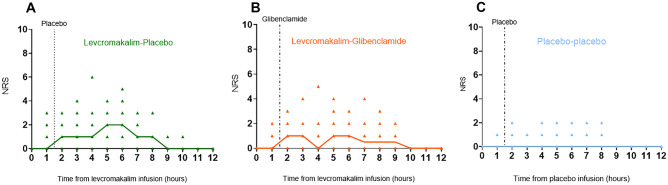
Intravenous infusion of ATP-sensitive potassium channel (K) opener levcromakalim causes headache in humans and implicates K channels in headache pathophysiology. Whether K channel blocker glibenclamide inhibits levcromakalim-induced headache has not yet been elucidated. We aimed to investigate the effect of posttreatment with glibenclamide on levcromakalim-induced headache in healthy participants. In a double blind, randomized, three-arm, placebo-controlled, crossover study, 20 healthy participants were randomized to receive 20 mL of levcromakalim (0.05 mg/min (50 mg/mL)) or 20 mL placebo (isotonic saline) intravenously over 20 min followed by oral administration of 10 mg glibenclamide or placebo. Fifteen participants completed all three study days. The primary endpoint was the difference in incidence of headache (0-12 h) between glibenclamide and placebo. More participants developed headache on levcromakalim-placebo day (15/15, 100%) (P = 0.013) and levcromakalim-glibenclamide day (13/15, 86%) compared to placebo-placebo day (7/15, 46%) (P = 0.041). We found no difference in headache incidence between levcromakalim-placebo day and levcromakalim-glibenclamide day (P = 0.479). The AUC for headache intensity was significantly larger in levcromakalim-placebo day and levcromakalim-glibenclamide day compared to placebo-placebo day (106.3 ± 215.8) (P < 0.01). There was no difference in the AUC for headache intensity between the levcromakalim-placebo day (494 ± 336.6) and the levcromakalim-glibenclamide day (417 ± 371.6) (P = 0.836). We conclude that non-specific K channel inhibitor glibenclamide did not attenuate levcromakalim-induced headache in healthy volunteers. Future studies should clarify the involvement of the distinct isoforms of sulfonylurea receptor subunits of K channels in the pathogenesis of headache and migraine.
静脉输注三磷酸腺苷敏感性钾通道 (K) 开放剂 levcromakalim 可引起人类头痛,并提示 K 通道参与头痛的病理生理学。K 通道阻滞剂格列本脲是否抑制 levcromakalim 引起的头痛尚未阐明。我们旨在研究健康参与者中格列本脲治疗后对 levcromakalim 引起的头痛的影响。在一项双盲、随机、三臂、安慰剂对照、交叉研究中,将 20 名健康参与者随机分为静脉输注 20 mL levcromakalim(0.05 mg/min(50 mg/mL))或 20 mL 安慰剂(等渗盐水),持续 20 分钟,然后口服 10 mg 格列本脲或安慰剂。15 名参与者完成了所有 3 天的研究。主要终点是格列本脲和安慰剂之间头痛(0-12 小时)发生率的差异。与安慰剂-安慰剂日(7/15,46%)相比,在 levcromakalim-安慰剂日(15/15,100%)(P=0.013)和 levcromakalim-格列本脲日(13/15,86%)中更多的参与者出现头痛(P=0.041)。我们发现 levcromakalim-安慰剂日和 levcromakalim-格列本脲日之间的头痛发生率无差异(P=0.479)。与安慰剂-安慰剂日相比,levcromakalim-安慰剂日和 levcromakalim-格列本脲日的头痛强度 AUC 显著更大(106.3±215.8)(P<0.01)。与 levcromakalim-安慰剂日(494±336.6)相比,levcromakalim-格列本脲日的头痛强度 AUC 无差异(417±371.6)(P=0.836)。我们的结论是,非特异性 K 通道抑制剂格列本脲并未减轻健康志愿者中 levcromakalim 引起的头痛。未来的研究应阐明不同的磺酰脲受体亚单位的 K 通道在头痛和偏头痛发病机制中的作用。