Department of Cardiovascular Medicine, The Second Xiangya Hospital of Central South University, No. 139 Middle Renmin Road, Furong District, Changsha City, 410011, Hunan Province, China.
BMC Pulm Med. 2023 Feb 11;23(1):62. doi: 10.1186/s12890-023-02355-1.
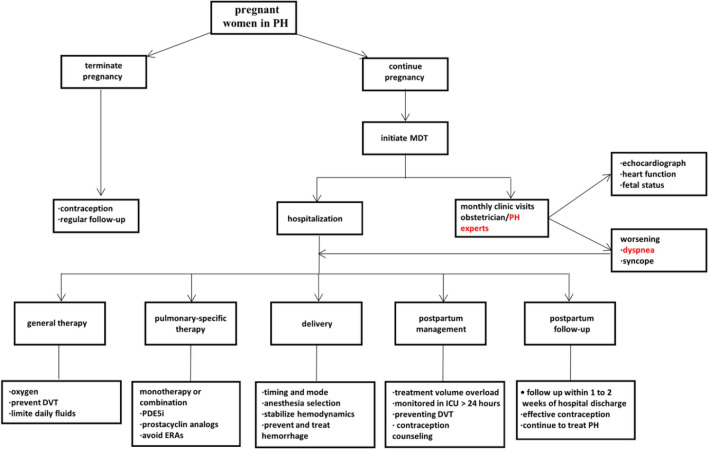
The importance of multidisciplinary team (MDT) centred on pregnant women with pulmonary hypertension (PH) has been highlighted. However, rare studies have explored its effects on pregnancy outcomes. This study seeks to investigate whether and how the MDT has an effect on the treatment and outcomes of PH pregnant women.
A pre- and post-intervention study was conducted based on an interrupted time series design to compare the treatment and outcomes of patients with PH before (pre-MDT) and after (post-MDT) implementation of the MDT. PH was defined as pulmonary artery systolic pressure (sPAP) ≥ 35 mmHg measured by echocardiography or right heart catheterization and sPAP at 35-60 mmHg and over 60 mmHg was defined as mild and severe PH, respectively. All results were analyzed by T-tests, Chi square tests or Fisher exact test and two-sided p value < 0.05 was set to be statistically significant.
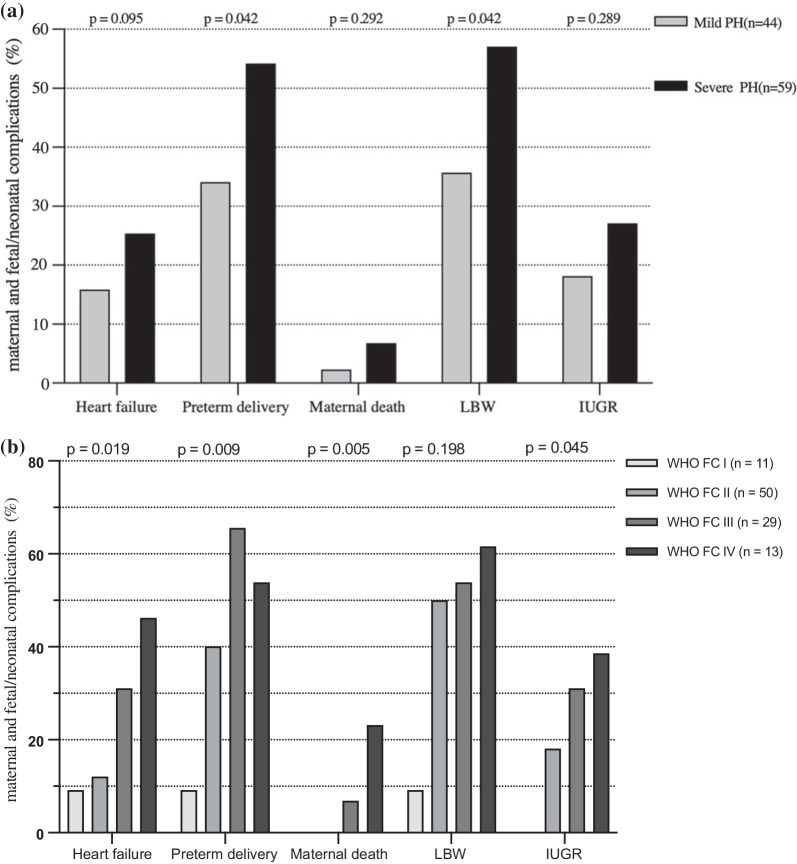
149 pregnancies were found in 143 women with PH. Overall, 46 pregnancies were elective abortions, remaining 49 and 54 pregnancies completing delivery in the pre-MDT group and post-MDT group, respectively. Five (10.2%) mother and seven (8.6%) neonatal died in the former, while no maternal deaths but 1.9% neonatal death occurred in the latter. In subgroup analysis, maternal and fetal/neonatal complications were higher in patients with severe PH and World Health Organization functional class (WHO FC) III/IV and all maternal deaths occurred in class III/IV women. In pre-MDT and post-MDT groups, there were 8 and 22 pregnant women receiving the pulmonary-specific therapy and completing delivery, respectively. The percentage of heart failure and urgent cesarean of pre-MDT group was higher than the post-MDT group (30.6% vs. 12.9%, p = 0.02; 40.8% vs. 14.8%, p = 0.01, respectively).
Implementing the MDT decreased the rate of urgent caesarean section and heart failure in patients with PH and no maternal deaths occurred in the post-MDT group. Pregnant women with severe PH and WHO FC III/IV might have a poor prognosis, whereas the use of pulmonary-specific therapy might improve outcomes of pregnancy.
以孕妇为中心的多学科团队(MDT)在肺动脉高压(PH)中的重要性已经得到强调。然而,很少有研究探讨其对妊娠结局的影响。本研究旨在探讨 MDT 是否以及如何影响 PH 孕妇的治疗和结局。
本研究采用前后对照的干预性研究设计,比较了 MDT 实施前后(MDT 前和 MDT 后)PH 患者的治疗和结局。PH 定义为超声心动图或右心导管检查测量的肺动脉收缩压(sPAP)≥35mmHg,sPAP 在 35-60mmHg 和超过 60mmHg 分别定义为轻度和重度 PH。所有结果均采用 T 检验、卡方检验或 Fisher 确切概率法进行分析,双侧 p 值<0.05 为统计学显著差异。
在 143 名 PH 妇女中发现了 149 例妊娠。总的来说,46 例妊娠为选择性流产,MDT 前组和 MDT 后组分别有 49 例和 54 例妊娠完成分娩。前者有 5 例(10.2%)母亲和 7 例(8.6%)新生儿死亡,后者无母亲死亡但有 1.9%新生儿死亡。在亚组分析中,重度 PH 和世界卫生组织功能分级(WHO FC)III/IV 的患者母婴并发症更高,所有母亲死亡均发生在 III/IV 级的妇女中。在 MDT 前组和 MDT 后组中,分别有 8 例和 22 例孕妇接受了肺特异性治疗并完成了分娩。MDT 前组心力衰竭和紧急剖宫产的比例高于 MDT 后组(30.6%比 12.9%,p=0.02;40.8%比 14.8%,p=0.01)。
实施 MDT 降低了 PH 患者紧急剖宫产和心力衰竭的发生率,MDT 后组无母亲死亡。重度 PH 和 WHO FC III/IV 的孕妇预后可能较差,而肺特异性治疗可能改善妊娠结局。