Zhang Xiaomin, Wu Jinming, Qiao Liangliang, Chen Lixuan, Chen Chaolin, Zhang Hui, Luo Rongcheng, Xiao Yang
Department of Hematology, Jinshazhou Hospital of Guangzhou University of Chinese Medicine, Guangzhou, China.
Institute of Clinical Medicine College, Guangzhou University of Chinese Medicine, Guangzhou, China.
Front Oncol. 2023 Jan 27;13:1008828. doi: 10.3389/fonc.2023.1008828. eCollection 2023.
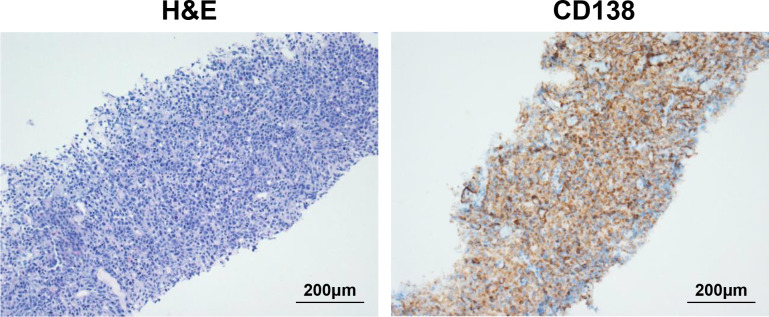
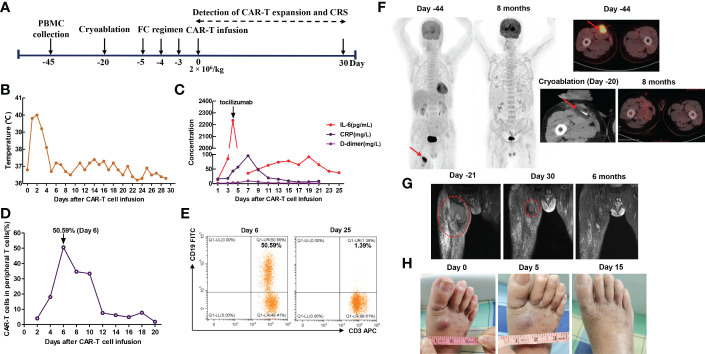
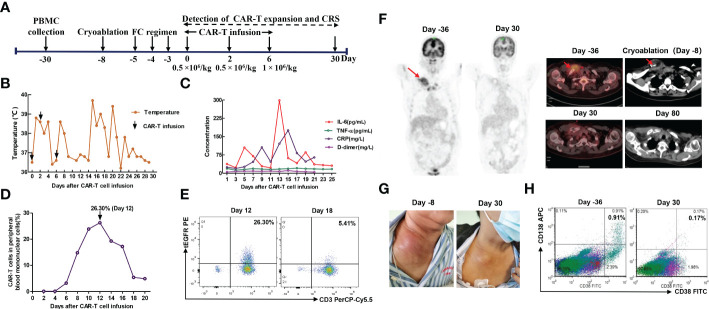
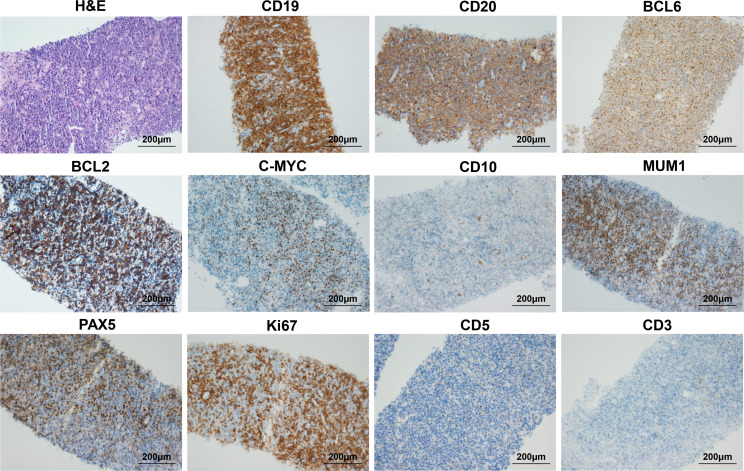
Chimeric antigen receptor (CAR) T-cell therapy has emerged as a powerful immunotherapy in relapsed/refractory (R/R) hematological malignancies, especially in R/R B-cell acute lymphocytic leukemia (B-ALL), non-Hodgkin lymphoma (NHL), and multiple myeloma (MM). To prevent disease progression and reduce tumor burden during CAR-T cell manufacturing, bridging therapies prior to CAR-T cell infusion are crucial. At present, it has been demonstrated that targeted therapy, radiotherapy and autologous stem cell transplantation (ASCT) could serve as effective bridging strategies. However, whether cryoablation could serve as a novel bridging strategy is unknown. In this paper, we report 2 cases of R/R B cell malignancies with bulky disease that were successfully treated with a combination of cryoablation and CAR-T cell therapy. Patient 1 was a 65-year-old female who was diagnosed with R/R MM with extramedullary disease (EMD). She was enrolled in the anti-BCMA CAR-T cell clinical trial. Patient 2 was a 70-year-old man who presented with a subcutaneous mass in the right anterior thigh and was diagnosed with primary cutaneous diffuse large B cell lymphoma, leg type (PCLBCL-LT) 1 year ago. He failed multiline chemotherapies as well as radiotherapy. Thus, he requested anti-CD19 CAR-T cell therapy. Unfortunately, they all experienced local progression during CAR-T cell manufacturing. To rapidly achieve local tumor control and reduce tumor burden, they both received cryoablation as a bridging therapy. Patient 1 achieved a very good partial response (VGPR) 1 month after CAR-T cell infusion, and patient 2 achieved a partial response (PR) 1 month after CAR-T cell infusion. In addition, adverse effects were tolerable and manageable. Our study demonstrated the favorable safety and efficacy of combination therapy with cryoablation and CAR-T cell therapy for the first time, and it also indicates that cryoablation could serve as a novel therapeutic strategy for local tumor control in B cell malignancies.
嵌合抗原受体(CAR)T细胞疗法已成为复发/难治性(R/R)血液系统恶性肿瘤,尤其是R/R B细胞急性淋巴细胞白血病(B-ALL)、非霍奇金淋巴瘤(NHL)和多发性骨髓瘤(MM)的一种强大免疫疗法。为防止疾病进展并在CAR-T细胞制造过程中减轻肿瘤负担,在CAR-T细胞输注前的桥接治疗至关重要。目前,已证明靶向治疗、放疗和自体干细胞移植(ASCT)可作为有效的桥接策略。然而,冷冻消融是否可作为一种新型桥接策略尚不清楚。在本文中,我们报告了2例R/R B细胞恶性肿瘤伴巨大肿块的病例,它们通过冷冻消融和CAR-T细胞疗法联合成功治疗。患者1是一名65岁女性,被诊断为伴有髓外疾病(EMD)的R/R MM。她参加了抗BCMA CAR-T细胞临床试验。患者2是一名70岁男性,1年前右大腿前侧出现皮下肿块,被诊断为原发性皮肤弥漫性大B细胞淋巴瘤,腿部型(PCLBCL-LT)。他多线化疗及放疗均失败。因此,他要求接受抗CD19 CAR-T细胞治疗。不幸的是,他们在CAR-T细胞制造过程中均出现局部进展。为迅速实现局部肿瘤控制并减轻肿瘤负担,他们都接受了冷冻消融作为桥接治疗。患者1在CAR-T细胞输注后1个月达到非常好的部分缓解(VGPR),患者2在CAR-T细胞输注后1个月达到部分缓解(PR)。此外,不良反应可耐受且可控。我们的研究首次证明了冷冻消融与CAR-T细胞疗法联合治疗的良好安全性和有效性,也表明冷冻消融可作为B细胞恶性肿瘤局部肿瘤控制的一种新型治疗策略。