Sharma Himanshu, McGinnis John P, Kabotyanski Katherine E, Gopinath Shankar P, Goodman Jerry C, Robertson Claudia, Cruz Navarro Jovany
Department of Neurosurgery, Baylor College of Medicine, Houston, TX, United States.
Baylor College of Medicine, Houston, TX, United States.
Front Neurol. 2023 Jan 27;14:1017290. doi: 10.3389/fneur.2023.1017290. eCollection 2023.
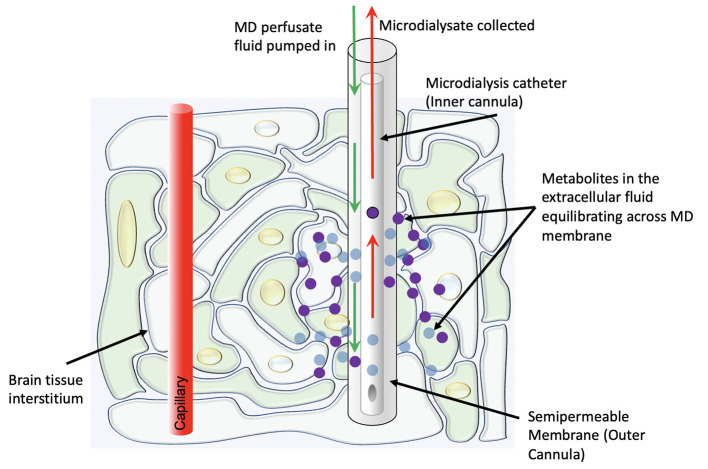
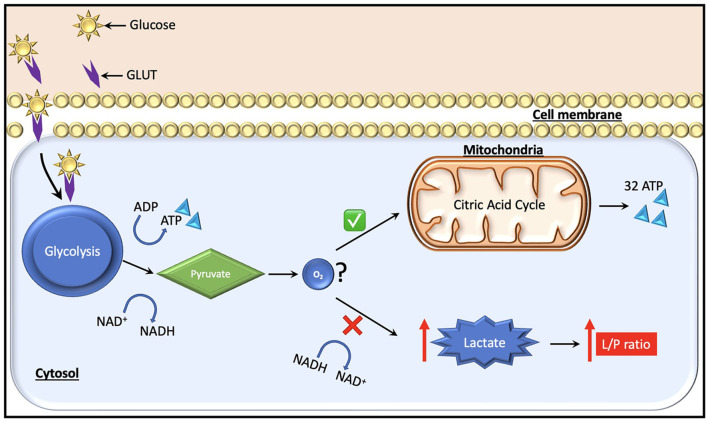
Traditionally, intracranial pressure (ICP) and partial brain tissue oxygenation (PbtO) have been the primary invasive intracranial measurements used to guide management in patients with severe traumatic brain injury (TBI). After injury however, the brain develops an increased metabolic demand which may require an increment in the oxidative metabolism of glucose. Simultaneously, metabolic, and electrical dysfunction can lead to an inability to meet these demands, even in the absence of ischemia or increased intracranial pressure. Cerebral microdialysis provides the ability to accurately measure local concentrations of various solutes including lactate, pyruvate, glycerol and glucose. Experimental and clinical data demonstrate that such measurements of cellular metabolism can yield critical missing information about a patient's physiologic state and help limit secondary damage. Glucose management in traumatic brain injury is still an unresolved question. As cerebral glucose metabolism may be uncoupled from systemic glucose levels due to the metabolic dysfunction, measurement of cerebral extracellular glucose concentrations could provide more predictive information and prove to be a better biomarker to avoid secondary injury of at-risk brain tissue. Based on data obtained from cerebral microdialysis, specific interventions such as ICP-directed therapy, blood glucose increment, seizure control, and/or brain oxygen optimization can be instituted to minimize or prevent secondary insults. Thus, microdialysis measurements of parenchymal metabolic function provides clinically valuable information that cannot be obtained by other monitoring adjuncts in the standard ICU setting.
传统上,颅内压(ICP)和脑组织局部氧合(PbtO)一直是用于指导重型创伤性脑损伤(TBI)患者治疗的主要有创性颅内测量指标。然而,受伤后,大脑的代谢需求增加,这可能需要增加葡萄糖的氧化代谢。同时,代谢和电功能障碍可能导致即使在没有缺血或颅内压升高的情况下也无法满足这些需求。脑微透析能够准确测量包括乳酸、丙酮酸、甘油和葡萄糖在内的各种溶质的局部浓度。实验和临床数据表明,这种细胞代谢测量可以提供有关患者生理状态的关键缺失信息,并有助于限制继发性损伤。创伤性脑损伤中的葡萄糖管理仍然是一个未解决的问题。由于代谢功能障碍,脑葡萄糖代谢可能与全身葡萄糖水平解偶联,测量脑细胞外葡萄糖浓度可以提供更多预测信息,并被证明是避免高危脑组织继发性损伤的更好生物标志物。基于从脑微透析获得的数据,可以采取特定的干预措施,如ICP导向治疗、血糖升高、癫痫控制和/或脑氧优化,以尽量减少或预防继发性损伤。因此,实质代谢功能的微透析测量提供了在标准重症监护病房环境中其他监测辅助手段无法获得的临床有价值信息。