Department of Medicine, University of Zimbabwe, Harare, Zimbabwe.
Department of Medicine, University of Stellenbosch, Cape Town, South Africa.
PLoS One. 2023 Feb 14;18(2):e0281279. doi: 10.1371/journal.pone.0281279. eCollection 2023.
In Zimbabwe, children, adolescents and young adults living with HIV (CALWH) who are on public health antiretroviral therapy (ART) have inadequate viral load (VL) suppression. We assessed whether a clinic-based VL monitoring could decrease 12-month virologic failure rates among these CALWH.
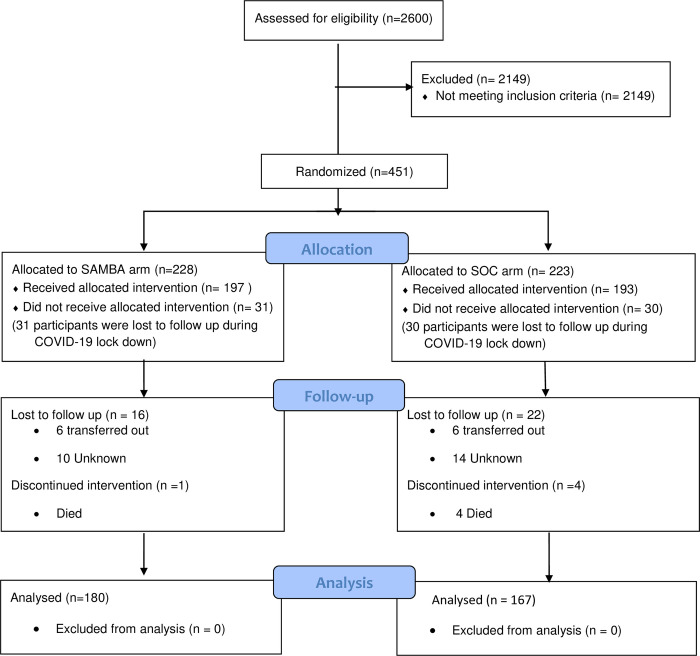
The study was registered on ClinicalTrials.gov: NCT03986099. CALWH in care at Chidamoyo Christian Hospital (CCH) and 8 rural outreach sites (ROS) on long-term community-based ART were randomized (1:1) to 6 monthly VL monitoring by COBAS®Ampliprep®/Taqman48® HIV-1 at the provincial referral laboratory (PRL) as per standard of care (SOC) or by the clinic-based SAMBA II assay, Diagnostics for the Real World, at CCH. VL suppression, turn-around-time (TAT) for VL results, drug switching and drug resistance in second-line failure were assessed at 12 months.
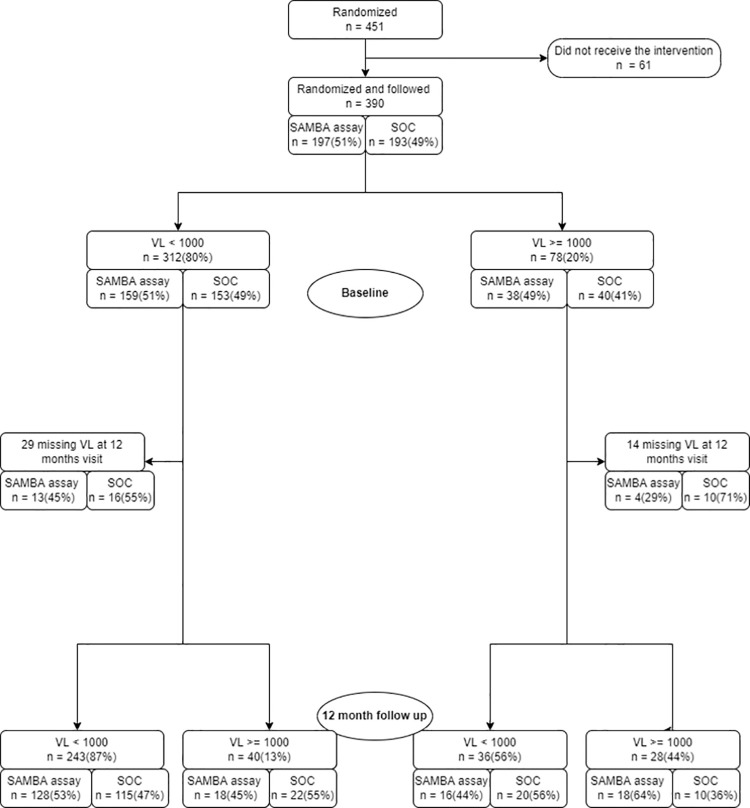
Of 390 CALWH enrolled 347 (89%) completed 12 months follow-up. Median (IQR) age and ART duration were 14.1 (9.7-18.2) and 6.4 (3.7-7.9) years, respectively. Over half (57%) of the participants were female. At enrolment, 78 (20%) had VL ≥1,000 copies/ml and VL suppression of 80% was unchanged after 12 months, with no significant difference between the SOC (81%) and the clinic-based (80%) arms (p = 0.528). Median (IQR) months to confirmatory VL result at CCH vs PRL was 4.0 (2.1-4.4) vs 4.5 (3.5-6.3) respectively; p = 0.027 at 12 months. Drug switching was documented among 26/347 (7%) participants with no difference between the median (IQR) time to switch in SOC vs clinic-based arms (5.1 (3.9-10.0) months vs 4.4 (2.5-8.4) respectively; p = 0.569). Out of 24 confirmed second-line failures, only 4/19 (21%) had protease inhibitor resistance.
In rural Zimbabwe, the clinic-based SAMBA II assay was able to provide confirmatory VL results faster than the SOC VL assay at the PRL. However, this rapid TAT did not allow for a more efficient drug switch among these CALWH.
在津巴布韦,接受公共卫生抗逆转录病毒疗法(ART)的儿童、青少年和青年艾滋病毒感染者(CALWH)的病毒载量(VL)抑制不足。我们评估了基于诊所的 VL 监测是否可以降低这些 CALWH 中 12 个月时的病毒学失败率。
该研究已在 ClinicalTrials.gov 上注册:NCT03986099。在长期社区为基础的 ART 中,在 Chidamoyo 基督教医院(CCH)和 8 个农村外展点(ROS)接受护理的 CALWH 按 1:1 随机分配(1:1)接受 COBAS®Ampliprep®/Taqman48® HIV-1 每 6 个月一次的 VL 监测,通过省级转介实验室(PRL)按标准护理(SOC)或通过诊所的 SAMBA II 检测,诊断现实世界,在 CCH。在 12 个月时评估 VL 抑制、VL 结果的周转时间(TAT)、药物转换和二线治疗失败的耐药性。
在纳入的 390 名 CALWH 中,有 347 名(89%)完成了 12 个月的随访。中位(IQR)年龄和 ART 持续时间分别为 14.1(9.7-18.2)和 6.4(3.7-7.9)年,分别。超过一半(57%)的参与者为女性。在入组时,有 78 名(20%)的 VL≥1000 拷贝/ml,VL 抑制率为 80%,12 个月后无变化,SOC(81%)和基于诊所的(80%)手臂之间没有显著差异(p=0.528)。在 CCH 与 PRL 分别确认 VL 结果的中位(IQR)时间分别为 4.0(2.1-4.4)个月和 4.5(3.5-6.3)个月;p=0.027,在 12 个月时。在 26/347(7%)的参与者中记录了药物转换,SOC 与基于诊所的手臂之间在中位(IQR)药物转换时间上没有差异(5.1(3.9-10.0)个月与 4.4(2.5-8.4)个月;p=0.569)。在 24 例确认的二线治疗失败中,只有 4/19(21%)有蛋白酶抑制剂耐药。
在津巴布韦农村地区,基于诊所的 SAMBA II 检测能够比 SOC 在 PRL 更快地提供确认性 VL 结果。然而,这种快速的 TAT 并没有使这些 CALWH 中的药物转换更有效率。