Department of Clinical and Experimental Medicine, University of Pisa, Pisa, Italy.
Laboratory of Metabolism, Nutrition, and Atherosclerosis, University of Pisa, Pisa, Italy.
Diabetes Care. 2023 Apr 1;46(4):845-853. doi: 10.2337/dc22-2003.
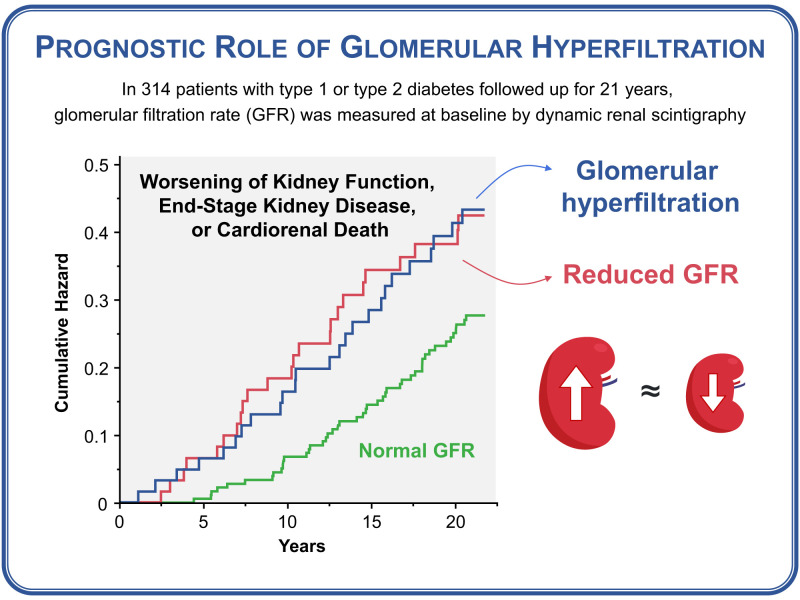
To evaluate the prognostic value of glomerular hyperfiltration on long-term kidney-related outcomes and mortality in patients with diabetes.
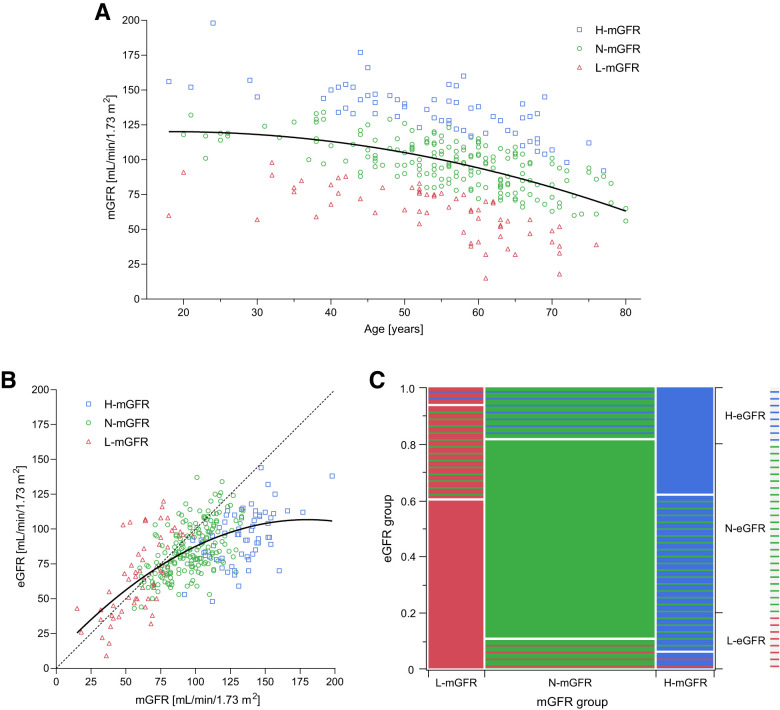
We retrospectively analyzed 21-year longitudinal data from 314 patients with long-standing type 1 or type 2 diabetes. Glomerular hyperfiltration was identified based on the age- and sex-specific distribution of measured glomerular filtration rate (mGFR) by 99mTc-DTPA dynamic renal scintigraphy. The primary outcome was a composite of doubling of serum creatinine, end-stage kidney disease (ESKD), or cardiorenal death. The kidney-specific outcome was a composite of doubling of serum creatinine, ESKD, or renal death.
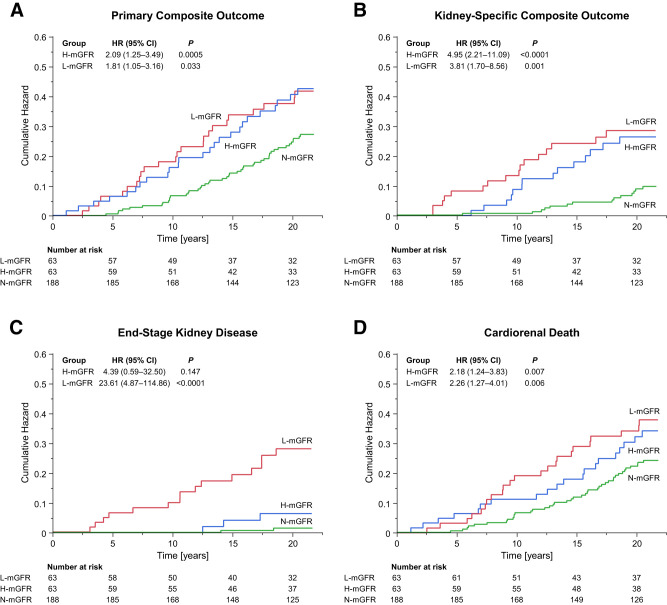
Over a median of 21.0 years, the primary composite outcome occurred in 25 (39.7%), 24 (38.1%), and 46 (24.5%) participants with high mGFR (H-mGFR) (n = 63), low mGFR (L-mGFR) (n = 63), or normal mGFR (N-mGFR) (n = 188), respectively. Compared with N-mGFR, the hazard ratio (HR) for the primary composite outcome was 2.09 (95% CI 1.25-3.49) in H-mGFR and 1.81 (1.05-3.16) in L-mGFR. The HR for the kidney-specific composite outcome was 4.95 (2.21-11.09) in H-mGFR and 3.81 (1.70-8.56) in L-mGFR. The HRs for doubling of serum creatinine and cardiorenal death were 4.86 (2.18-10.90) and 2.18 (1.24-3.83) in H-mGFR and 4.04 (1.77-9.20) and 2.26 (1.27-4.01) in L-mGFR, respectively.
Glomerular hyperfiltration, similar to hypofiltration, increases the combined risk of worsening kidney function and mortality from cardiovascular or renal causes in patients with diabetes. These findings encourage the active screening of these patients to optimize risk stratification and treatment of subclinical kidney disease.
评估糖尿病患者肾小球高滤过对长期肾脏相关结局和死亡率的预后价值。
我们回顾性分析了 314 例长期 1 型或 2 型糖尿病患者 21 年的纵向数据。肾小球高滤过是根据 99mTc-DTPA 动态肾闪烁扫描测定的肾小球滤过率(mGFR)的年龄和性别特异性分布来确定的。主要结局是血清肌酐加倍、终末期肾病(ESKD)或心肾死亡的复合结局。肾脏特异性结局是血清肌酐加倍、ESKD 或肾脏死亡的复合结局。
在中位数为 21.0 年的随访中,高 mGFR(H-mGFR)(n=63)、低 mGFR(L-mGFR)(n=63)和正常 mGFR(N-mGFR)(n=188)参与者中,主要复合结局分别发生在 25 例(39.7%)、24 例(38.1%)和 46 例(24.5%)。与 N-mGFR 相比,H-mGFR 的主要复合结局的风险比(HR)为 2.09(95%CI 1.25-3.49),L-mGFR 的 HR 为 1.81(1.05-3.16)。H-mGFR 肾脏特异性复合结局的 HR 为 4.95(2.21-11.09),L-mGFR 的 HR 为 3.81(1.70-8.56)。H-mGFR 中血清肌酐加倍和心肾死亡的 HR 分别为 4.86(2.18-10.90)和 2.18(1.24-3.83),L-mGFR 中分别为 4.04(1.77-9.20)和 2.26(1.27-4.01)。
与低滤过相似,肾小球高滤过增加了糖尿病患者肾功能恶化和心血管或肾脏原因导致的死亡率的联合风险。这些发现鼓励对这些患者进行积极筛查,以优化亚临床肾脏疾病的风险分层和治疗。