From the UCSF Weill Institute for Neurosciences and Department of Neurology, University of California, San Francisco (S.L.H.); Department of Neurology and Center for Neuroinflammation and Experimental Therapeutics (A.B.-O.), Perelman School of Medicine, University of Pennsylvania, Philadelphia; Institute of Neuropathology and Department of Neurology (M.S.W.), Universitätsmedizin Göttingen Fraunhofer-Institute for Translational Medicine and Pharmacology ITMP, Göttingen, Germany; F. Hoffmann-La Roche Ltd (H. Kletzl, A.G., M.M., F. Model, F. Mercier, C.P., Q.W., H. Koendgen), Basel, Switzerland; NeuMatRx Ltd (T.S.), Bath, UK; and University Hospital Basel (L.K.), University of Basel, Switzerland.
Neurol Neuroimmunol Neuroinflamm. 2023 Feb 15;10(2). doi: 10.1212/NXI.0000000000200094. Print 2023 Mar.
Ocrelizumab improved clinical and MRI measures of disease activity and progression in three phase 3 multiple sclerosis (MS) studies. Post hoc analyses demonstrated a correlation between the ocrelizumab serum concentration and the degree of blood B-cell depletion, and body weight was identified as the most influential covariate on ocrelizumab pharmacokinetics. The magnitude of ocrelizumab treatment benefit on disability progression was greater in lighter vs heavier patients. These observations suggest that higher ocrelizumab serum levels provide more complete B-cell depletion and a greater delay in disability progression. The current post hoc analyses assessed population exposure-efficacy/safety relationships of ocrelizumab in patients with relapsing and primary progressive MS.
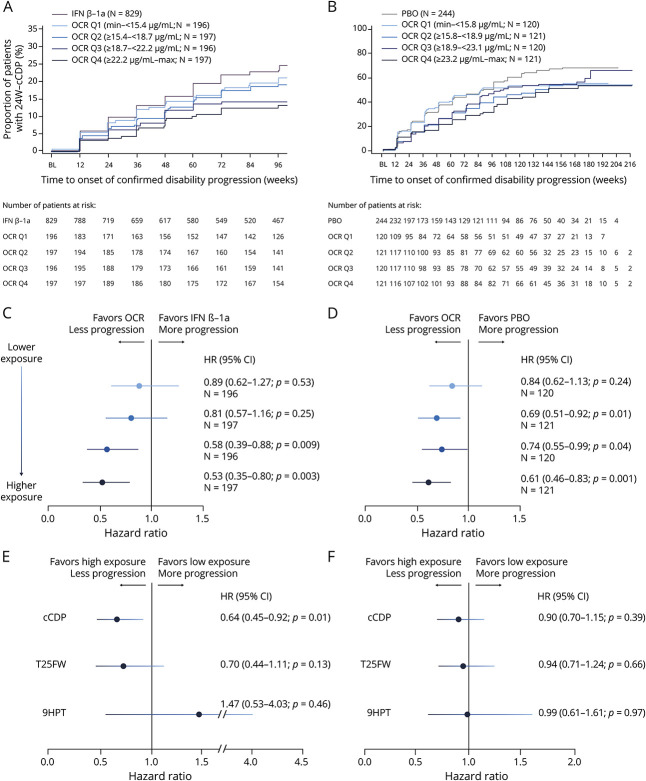
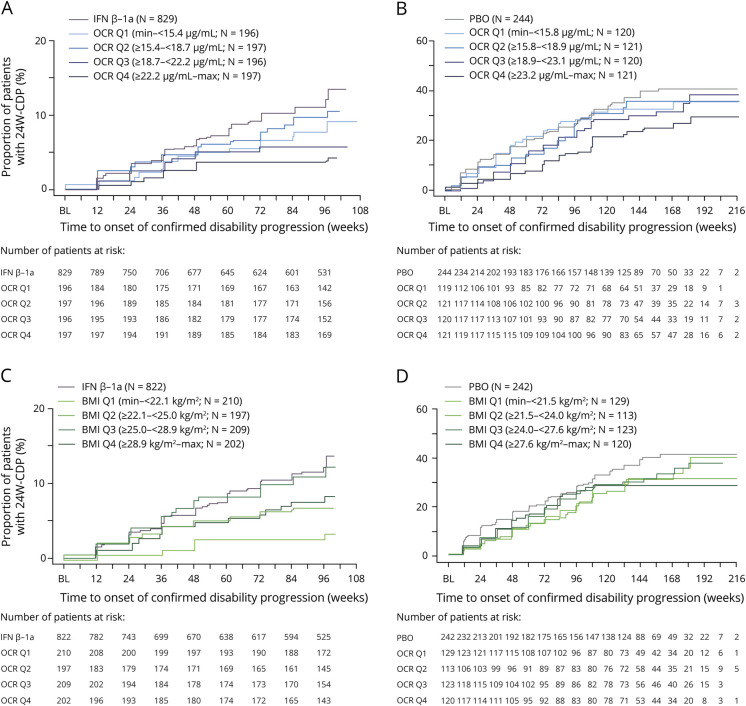
Patients in OPERA I/II and ORATORIO were grouped in exposure quartiles based on their observed individual serum ocrelizumab level over the treatment period. Exposure-response relationships were analyzed for clinical efficacy (24-week confirmed disability progression (CDP), annualized relapse rate [ARR], and MRI outcomes) and adverse events.
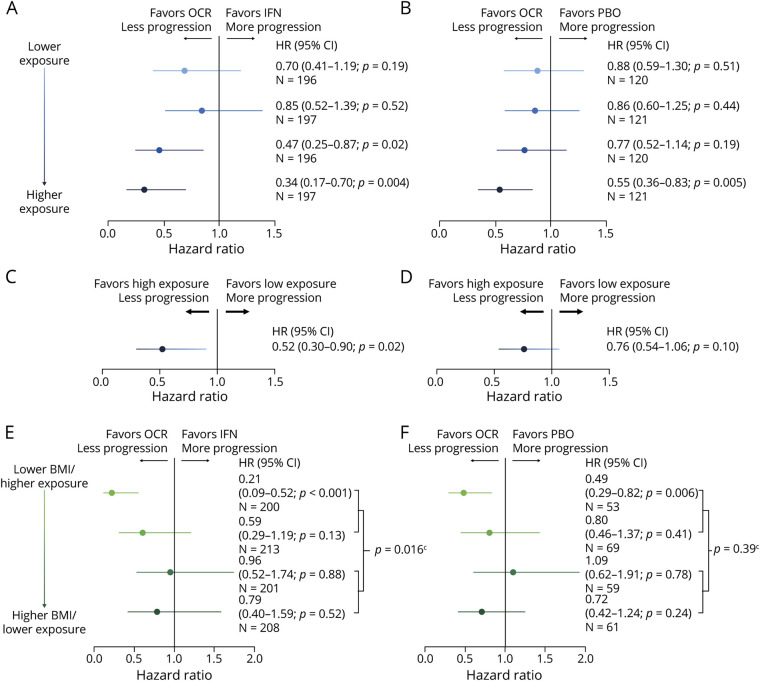
Ocrelizumab reduced new MRI lesion counts to nearly undetectable levels in patients with relapsing or primary progressive MS across all exposure subgroups, and reduced ARR in patients with relapsing MS to very low levels (0.13-0.18). A consistent trend of higher ocrelizumab exposure leading to lower rates of CDP was seen (0%-25% [lowest] to 75%-100% [highest] quartile hazard ratios and 95% confidence intervals; relapsing MS: 0.70 [0.41-1.19], 0.85 [0.52-1.39], 0.47 [0.25-0.87], and 0.34 [0.17-0.70] vs interferon β-1a; primary progressive MS: 0.88 [0.59-1.30], 0.86 [0.60-1.25], 0.77 [0.52-1.14], and 0.55 [0.36-0.83] vs placebo). Infusion-related reactions, serious adverse events, and serious infections were similar across exposure subgroups.
The almost complete reduction of ARR and MRI activity already evident in the lowest quartile, and across all ocrelizumab-exposure groups, suggests a ceiling effect. A consistent trend of higher ocrelizumab exposure leading to greater reduction in risk of CDP was observed, particularly in the relapsing MS trials, and was not associated with a higher rate of adverse events. Higher ocrelizumab exposure may provide improved control of disability progression by reducing disease activity below that detectable by ARR and MRI, and/or by attenuating other B-cell-related pathologies responsible for tissue damage.
This analysis provides Class III evidence that higher ocrelizumab serum levels are related to greater reduction in risk of disability progression in patients with multiple sclerosis. The study is rated Class III because of the initial treatment randomization disclosure that occurred after inclusion in the open-label extension.
ClinicalTrials.gov Identifier: NCT01247324 (OPERA I), NCT01412333 (OPERA II), and NCT01194570 (ORATORIO).
奥瑞珠单抗在三项 3 期多发性硬化症(MS)研究中改善了疾病活动度和进展的临床和 MRI 指标。事后分析表明,奥瑞珠单抗血清浓度与血液 B 细胞耗竭程度之间存在相关性,体重被确定为对奥瑞珠单抗药代动力学影响最大的协变量。在较轻的患者中,奥瑞珠单抗治疗对残疾进展的获益程度大于较重的患者。这些观察结果表明,较高的奥瑞珠单抗血清水平提供了更完全的 B 细胞耗竭,并在残疾进展方面延迟了更长的时间。目前的事后分析评估了奥瑞珠单抗在复发型和原发进展型 MS 患者中的人群暴露-疗效/安全性关系。
OPERA I/II 和 ORATORIO 中的患者根据其在治疗期间观察到的个体奥瑞珠单抗血清水平,分为暴露四分位数组。对临床疗效(24 周确认的残疾进展(CDP)、年复发率(ARR)和 MRI 结果)和不良事件进行了暴露-反应关系分析。
奥瑞珠单抗使复发型或原发进展型 MS 患者的新 MRI 病变计数几乎降至无法检测的水平,且使复发型 MS 患者的 ARR 降至极低水平(0.13-0.18)。在所有暴露亚组中,奥瑞珠单抗暴露水平较高与 CDP 发生率较低呈一致趋势(0%-25%[最低]至 75%-100%[最高]四分位数风险比和 95%置信区间;复发型 MS:0.70[0.41-1.19]、0.85[0.52-1.39]、0.47[0.25-0.87]和 0.34[0.17-0.70] 与干扰素β-1a 相比;原发进展型 MS:0.88[0.59-1.30]、0.86[0.60-1.25]、0.77[0.52-1.14]和 0.55[0.36-0.83] 与安慰剂相比)。输注相关反应、严重不良事件和严重感染在各暴露亚组中相似。
在最低四分位数中已经观察到 ARR 和 MRI 活动的几乎完全降低,并且在所有奥瑞珠单抗暴露组中,这表明存在一个上限效应。观察到奥瑞珠单抗暴露水平较高与 CDP 风险降低程度较大呈一致趋势,尤其是在复发型 MS 试验中,且与不良事件发生率增加无关。较高的奥瑞珠单抗暴露可能通过降低疾病活动度来改善残疾进展的控制,这种疾病活动度低于 ARR 和 MRI 可检测到的水平,并且/或者通过减轻其他与 B 细胞相关的导致组织损伤的病理学。
本分析提供了 III 类证据,表明多发性硬化症患者中较高的奥瑞珠单抗血清水平与残疾进展风险降低程度更大相关。该研究被评为 III 类,因为最初的治疗随机化披露是在开放标签扩展纳入后发生的。
ClinicalTrials.gov 标识符:NCT01247324(OPERA I)、NCT01412333(OPERA II)和 NCT01194570(ORATORIO)。