Division of Hematology, Diabetes, and Endocrinology, Department of Internal Medicine, Faculty of Medicine, University of Miyazaki, Miyazaki.
Division of Hematology, Department of Medicine, Keio University School of Medicine, Tokyo, Japan; Division of Molecular Oncology, National Cancer Center Research Institute, Tokyo.
Haematologica. 2023 Aug 1;108(8):2178-2191. doi: 10.3324/haematol.2022.281510.
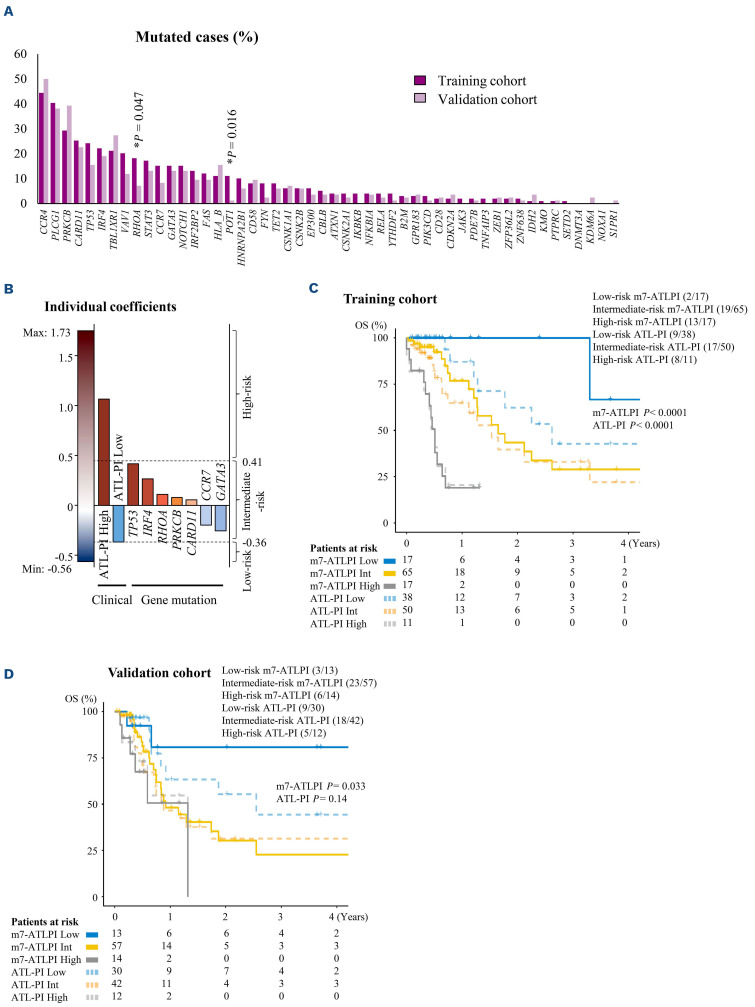
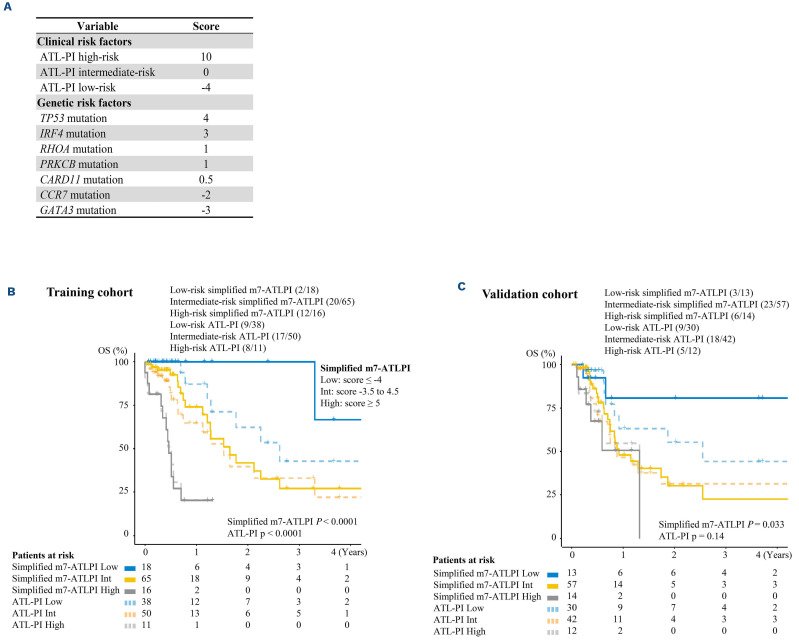
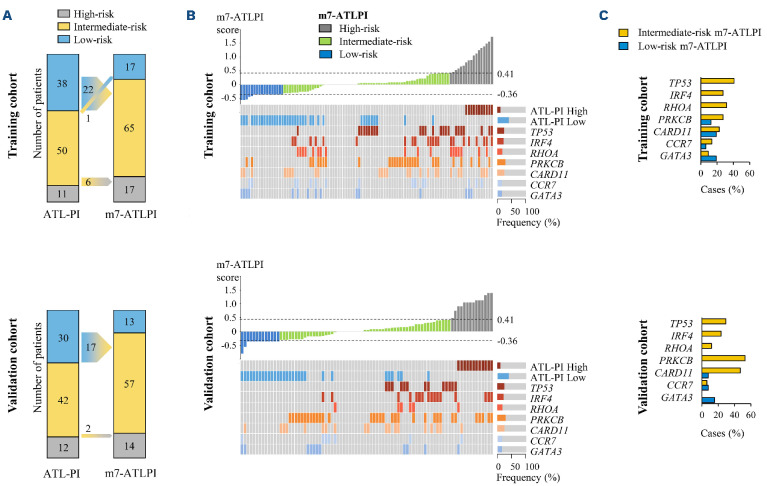
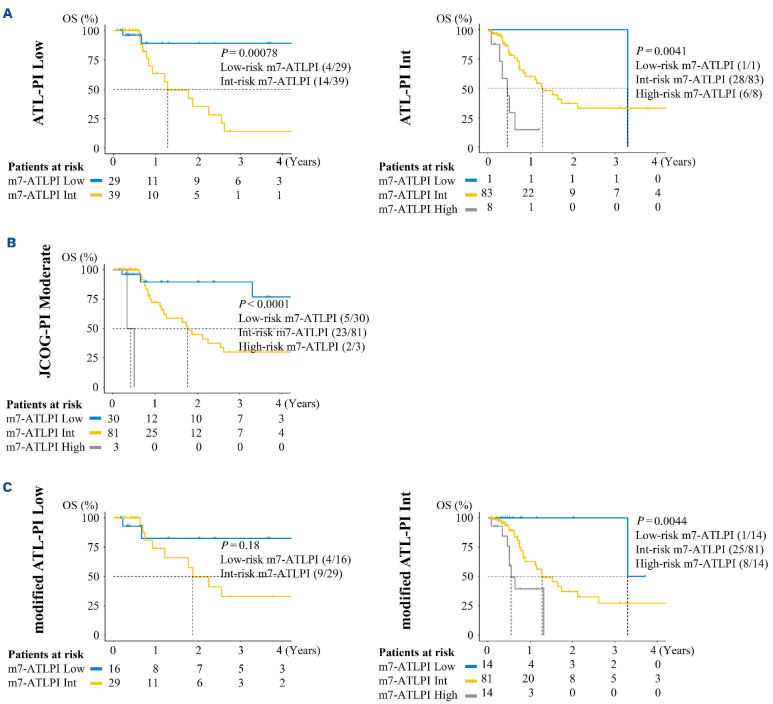
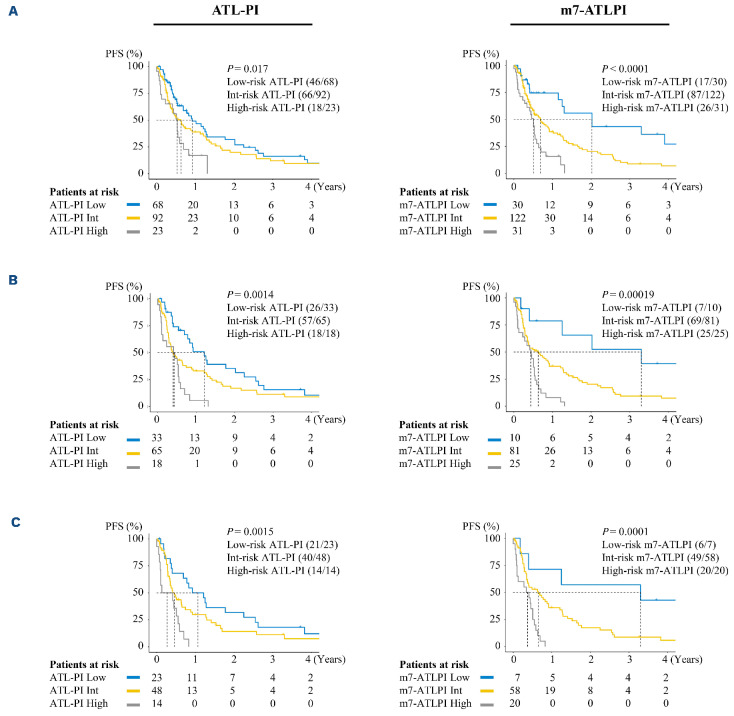
The prognosis of aggressive adult T-cell leukemia/lymphoma (ATL) is poor, and allogeneic hematopoietic stem cell transplantation (allo-HSCT) is a curative treatment. In order to identify favorable prognostic patients after intensive chemotherapy, and who therefore might not require upfront allo-HSCT, we aimed to improve risk stratification of aggressive ATL patients aged <70 years. The clinical risk factors and genetic mutations were incorporated into risk modeling for overall survival (OS). We generated the m7-ATLPI, a clinicogenetic risk model for OS, that included the ATL prognostic index (PI) (ATL-PI) risk category, and non-silent mutations in seven genes, namely TP53, IRF4, RHOA, PRKCB, CARD11, CCR7, and GATA3. In the training cohort of 99 patients, the m7-ATLPI identified a low-, intermediate-, and highrisk group with 2-year OS of 100%, 43%, and 19%, respectively (hazard ratio [HR] =5.46; P<0.0001). The m7-ATLPI achieved superior risk stratification compared to the current ATL-PI (C-index 0.92 vs. 0.85, respectively). In the validation cohort of 84 patients, the m7-ATLPI defined low-, intermediate-, and high-risk groups with a 2-year OS of 81%, 30%, and 0%, respectively (HR=2.33; P=0.0094), and the model again outperformed the ATL-PI (C-index 0.72 vs. 0.70, respectively). The simplified m7-ATLPI, which is easier to use in clinical practice, achieved superior risk stratification compared to the ATLPI, as did the original m7-ATLPI; the simplified version was calculated by summing the following: high-risk ATL-PI category (+10), low-risk ATL-PI category (-4), and non-silent mutations in TP53 (+4), IRF4 (+3), RHOA (+1), PRKCB (+1), CARD11 (+0.5), CCR7 (-2), and GATA3 (-3).
侵袭性成人 T 细胞白血病/淋巴瘤(ATL)的预后较差,异基因造血干细胞移植(allo-HSCT)是一种治愈性治疗方法。为了确定强化化疗后预后良好且可能不需要 upfront allo-HSCT 的患者,我们旨在改善<70 岁侵袭性 ATL 患者的风险分层。将临床危险因素和基因突变纳入总体生存(OS)风险模型中。我们生成了 m7-ATLPI,这是一个用于 OS 的临床遗传学风险模型,其中包括 ATL 预后指数(PI)(ATL-PI)风险类别,以及七个基因中的非沉默突变,即 TP53、IRF4、RHOA、PRKCB、CARD11、CCR7 和 GATA3。在 99 例患者的训练队列中,m7-ATLPI 将患者分为低危、中危和高危组,其 2 年 OS 分别为 100%、43%和 19%(风险比[HR] =5.46;P<0.0001)。m7-ATLPI 的风险分层优于当前的 ATL-PI(C 指数分别为 0.92 和 0.85)。在 84 例患者的验证队列中,m7-ATLPI 将患者分为低危、中危和高危组,其 2 年 OS 分别为 81%、30%和 0%(HR=2.33;P=0.0094),模型再次优于 ATL-PI(C 指数分别为 0.72 和 0.70)。更简单的 m7-ATLPI 更便于在临床实践中使用,与 ATL-PI 相比,简化版和原始版都能实现更好的风险分层;简化版的计算方法是将高危 ATL-PI 类别(+10)、低危 ATL-PI 类别(-4)、TP53、IRF4、RHOA、PRKCB、CARD11、CCR7 和 GATA3 中的非沉默突变(分别为+4、+3、+1、+1、+0.5、-2 和-3)相加。