Abdollahi Sara, Hadizadeh Yazdi Mohammad Hadi, Mowlavi Ali Asghar, Ceberg Sofie, Aznar Marianne Camille, Tabrizi Fatemeh Varshoee, Salek Roham, Ghodsi Alireza, Shams Ali
Physics Department, Faculty of Science, Ferdowsi University of Mashhad, Mashhad, Iran.
Medical Physics Department, Reza Radiotherapy and Oncology Center, Mashhad, Iran.
Tech Innov Patient Support Radiat Oncol. 2023 Jan 26;25:100201. doi: 10.1016/j.tipsro.2023.100201. eCollection 2023 Mar.
To investigate the possibility to be able to offer left sided breast cancer patients, not suitable for DIBH, an organ at risk saving treatment.
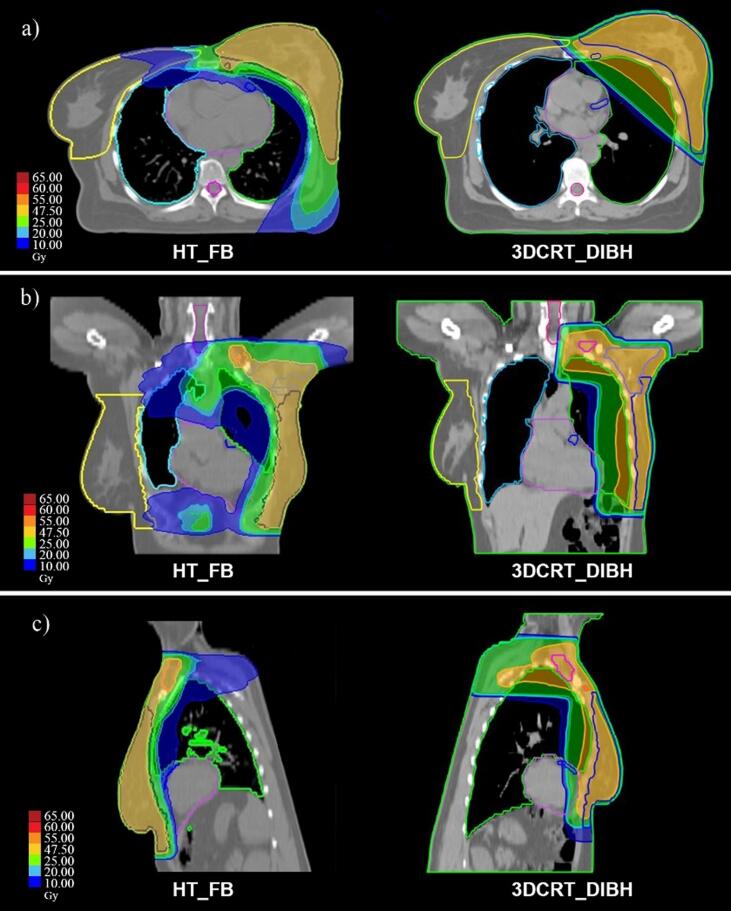
Twenty patients receiving radiotherapy for left breast cancer in DIBH were enrolled in the study. Planning CT scans were acquired in the same supine treatment position in FB and DIBH. 3DCRT_DIBH plans were designed and optimized using two parallel opposed tangent beams (with some additional segments) for the breast and chest wall and anterior-posterior fields for regional lymph nodes irradiation. Additionally, FB helical tomotherapy plans were optimized to minimize heart and lung dose. All forty plans were optimized with at least 95% of the total CTV covered by the 95% of prescribed dose of 50 Gy in 25 fractions.
HT_FB plans showed significantly better dose homogeneity and conformity compared to the 3DCRT_DIBH specially for regional nodal irradiation. The heart mean dose was almost comparable in 3DCRT_DIBH and HT_FB while the volume (%) of the heart receiving 25 Gy had a statistically significant reduction from 7.90 ± 3.33 in 3DCRT_DIBH to 0.88 ± 0.66 in HT_FB. HT_FB was also more effective in left descending artery (LAD) mean dose reduction about 100% from 30.83 ± 9.2 Gy to 9.7 ± 3.1. The ipsilateral lung volume receiving 20 Gy has a further reduction of 43 % in HT_FB compared with 3DCRT_DIBH. For low dose comparison, 3DCRT_DIBH was superior for contralateral organ sparing compared to the HT_FB due to the limited angle for dose delivery.
For patients who cannot be a candidate for DIBH for any reason, HT in free breathing may be a good alternative and provides heart and ipsilateral lung dose sparing, however with the cost of increased dose to contralateral breast and lung.
探讨为不适合深吸气屏气(DIBH)的左侧乳腺癌患者提供保危器官治疗的可能性。
20例接受左侧乳腺癌DIBH放疗的患者纳入本研究。在自由呼吸(FB)和DIBH状态下,于相同仰卧位治疗体位获取计划CT扫描图像。使用两平行对置切线野(加一些附加射野分段)对乳腺和胸壁进行3DCRT_DIBH计划设计及优化,并使用前后野对区域淋巴结进行照射。此外,对FB螺旋断层放疗计划进行优化以尽量减少心脏和肺的受量。所有40个计划均进行优化,使总临床靶体积(CTV)的至少95%被25次分割、50 Gy的处方剂量的95%覆盖。
与3DCRT_DIBH相比,HT_FB计划显示出显著更好的剂量均匀性和适形度,特别是对于区域淋巴结照射。3DCRT_DIBH和HT_FB的心脏平均剂量几乎相当,而接受25 Gy照射的心脏体积百分比从3DCRT_DIBH的7.90±3.33有统计学显著降低至HT_FB的0.88±0.66。HT_FB在降低左冠状动脉前降支(LAD)平均剂量方面也更有效,从30.83±9.2 Gy降低约100%至9.7±3.1 Gy。与3DCRT_DIBH相比,HT_FB中接受20 Gy照射的同侧肺体积进一步减少43%。对于低剂量比较,由于剂量投照角度受限,3DCRT_DIBH在对侧器官保护方面优于HT_FB。
对于因任何原因不适合DIBH的患者,自由呼吸状态下的螺旋断层放疗可能是一种良好的替代方案,并可实现心脏和同侧肺的剂量保护,然而代价是对侧乳腺和肺的剂量增加。