Department of Orthopaedic Surgery, Faculty of Medicine and Graduate School of Medicine, Hokkaido University, Kita-15 Nishi-7, Kita-Ku, Sapporo, 060-8638, Japan.
Department of Orthopaedic Surgery, Hakodate Central General Hospital, Hakodate, Hon-cho 33-2, 040-8585, Japan.
BMC Musculoskelet Disord. 2023 Feb 20;24(1):134. doi: 10.1186/s12891-023-06240-0.
This study compared the re-revision rate and radiographic outcomes of revision total hip arthroplasty (THA) using a Kerboull-type acetabular reinforcement device (KT plate) with bulk structural allograft and metal mesh with impaction bone grafting (IBG).
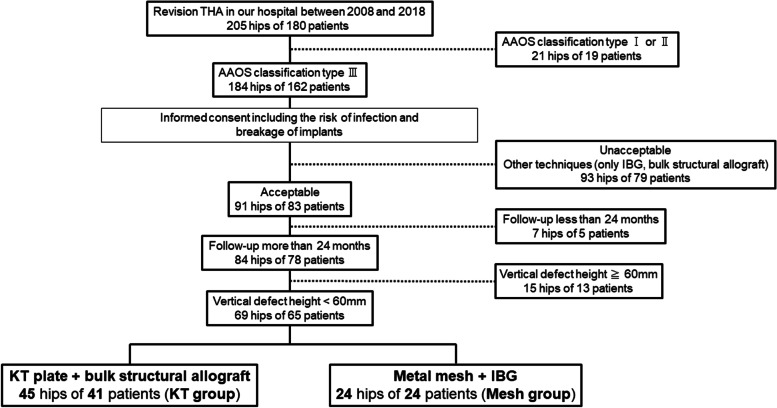
Ninety-one hips of 81 patients underwent revision THA for American Academy of Orthopedic Surgeons (AAOS) classification type III defects from 2008 to 2018. Of these, seven hips of five patients and 15 hips of 13 patients were excluded due to insufficient follow-up information (< 24 months) and large bone defects with a vertical defect height ≥ 60 mm, respectively. The current study compared the survival and radiographic parameters of 45 hips of 41 patients using a KT plate (KT group) and 24 hips of 24 patients using a metal mesh with IBG (mesh group).
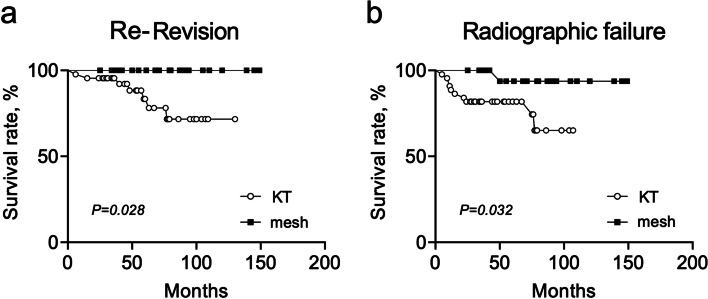
Eleven hips (24.4%) in the KT group and 1 hip (4.2%) in the mesh group exhibited radiological failure. Moreover, 8 hips in the KT group (17.0%) required a re-revision THA, while none of the patients in the mesh group required a re-revision. The survival rate with radiographic failure as the endpoint in the mesh group was significantly higher than that in the KT group (100% vs 86.7% at 1-year and 95.8% vs 80.0% at 5-years, respectively; p = 0.032). On multivariable analysis evaluating factors associated with radiographic failure, there were no significant associations with any radiographic measurement. Of the 11 hips with radiographic failure, 1 (11.1%), 3 (12.5%), and 7 (58.3%) hips were of Kawanabe classification stages 2, 3, and 4, respectively.
The findings of this study suggest that revision THA using KT plates with bulk structure allografts could provide poorer clinical outcomes than revision THA using a metal mesh with IBG. Although revision THA using KT plates with bulk structural allografts could set the true hip center, there is no association between a high hip center and clinical outcomes. The relationship between the position of the KT plate and the host bone might be considered more carefully.
本研究比较了 Kerboull 型髋臼加强装置(KT 板)联合结构性同种异体骨与金属网联合打压植骨在翻修全髋关节置换术(THA)中的再翻修率和影像学结果,后者用于治疗美国矫形外科医师学会(AAOS)分类 III 型髋臼缺损。
2008 年至 2018 年,81 例患者的 91 髋接受了翻修 THA,其中 7 髋(5 例)和 15 髋(13 例)由于随访信息不足(<24 个月)和垂直骨缺损高度≥60mm的大骨缺损而被排除在外。本研究比较了 45 髋(41 例)使用 KT 板(KT 组)和 24 髋(24 例)使用金属网联合打压植骨(网组)的患者的生存情况和影像学参数。
KT 组中有 11 髋(24.4%)和网组中有 1 髋(4.2%)出现影像学失败。此外,KT 组中有 8 髋(17.0%)需要再次翻修 THA,而网组中无一例患者需要再次翻修。以影像学失败为终点,网组的生存率明显高于 KT 组(1 年时为 100% vs. 86.7%,5 年时为 95.8% vs. 80.0%;p=0.032)。多变量分析评估与影像学失败相关的因素时,与任何影像学测量均无显著相关性。在 11 例影像学失败的患者中,1 髋(11.1%)、3 髋(12.5%)和 7 髋(58.3%)分别为 Kawanabe 分期 2 期、3 期和 4 期。
本研究结果表明,与金属网联合打压植骨的翻修 THA 相比,使用 KT 板联合结构性同种异体骨的翻修 THA 可能提供较差的临床结果。尽管使用 KT 板联合结构性同种异体骨的翻修 THA 可以重建真臼中心,但高臼中心与临床结果之间并无关联。KT 板与宿主骨之间的关系可能需要更仔细地考虑。