Godbout K, Bhutani M, Connors L, Chan C K N, Connors C, Dorscheid D, Dyck G, Foran V, Kaplan A G, Reynolds J, Waserman S
Quebec Heart and Lung Institute, Laval University, Quebec City, Canada.
Department of Medicine, Division of Pulmonary Medicine, University of Alberta, Western Canada, Edmonton, AB, Canada.
Allergy Asthma Clin Immunol. 2023 Feb 17;19(1):12. doi: 10.1186/s13223-023-00767-6.
In Canada, severe asthma affects an estimated 5-10% of people with asthma and is associated with frequent exacerbations, poor symptom control and significant morbidity from the disease itself, as well as the high dose inhaled, and systemic steroids used to treat it. Significant heterogeneity exists in service structure and patient access to severe asthma care, including access to biologic treatments. There appears to be over-reliance on short-acting beta agonists and frequent oral corticosteroid use, two indicators of uncontrolled asthma which can indicate undiagnosed or suboptimally treated severe asthma. The objective of this modified Delphi consensus project was to define standards of care for severe asthma in Canada, in areas where the evidence is lacking through patient and healthcare professional consensus, to complement forthcoming guidelines.
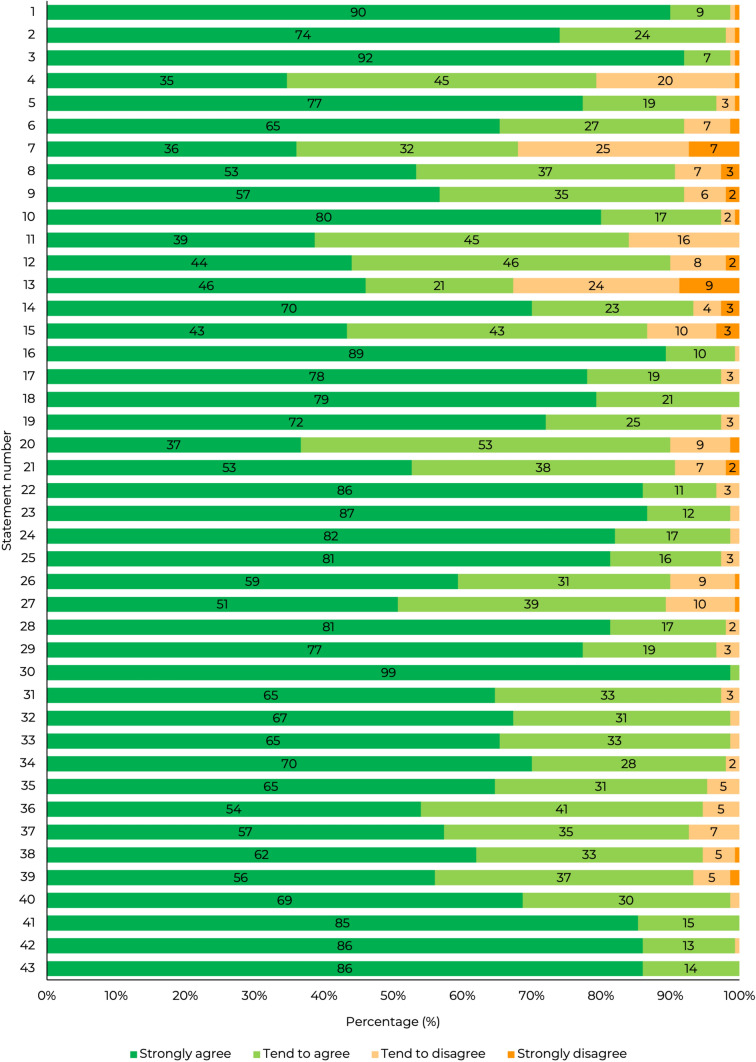
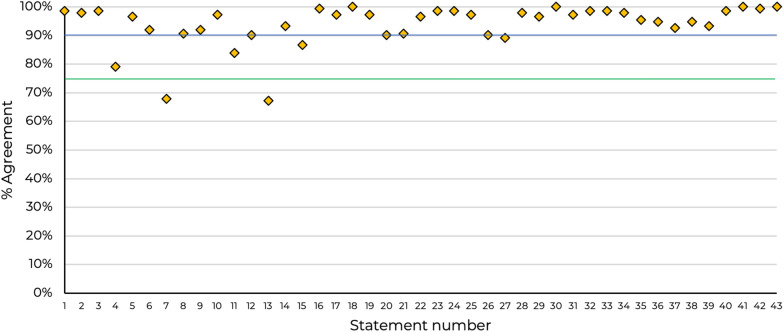
The steering group of asthma experts identified 43 statements formed from eight key themes. An online 4-point Likert scale questionnaire was sent to healthcare professionals working in asthma across Canada to assess agreement (consensus) with these statements. Consensus was defined as high if ≥ 75% and very high if ≥ 90% of respondents agreed with a statement.
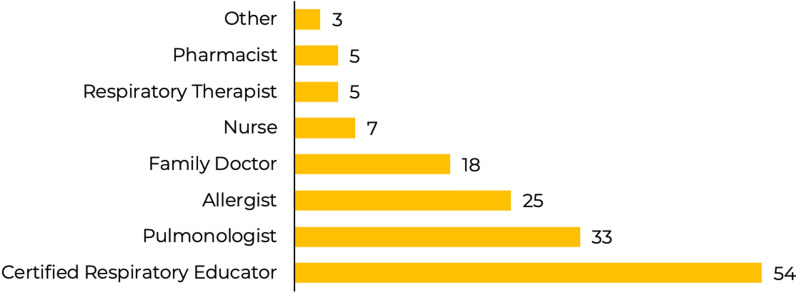
A total of 150 responses were received from HCPs including certified respiratory educators, respirologists, allergists, general practitioners/family physicians, nurses, pharmacists, and respiratory therapists. Consensus amongst respondents was very high in 37 (86%) statements, high in 4 (9%) statements and was not achieved in 2 (5%) statements. Based on the consensus scores, ten key recommendations were proposed. These focus on referrals from primary and secondary care, accessing specialist asthma services, homecare provision for severe asthma patients and outcome measures.
Implementation of these recommendations across the severe asthma care pathway in Canada has the potential to improve outcomes for patients through earlier detection of undiagnosed severe asthma, reduction in time to severe asthma diagnosis, and initiation of advanced phenotype specific therapies.
在加拿大,重度哮喘估计影响5%-10%的哮喘患者,与频繁发作、症状控制不佳以及疾病本身导致的显著发病率相关,同时也与用于治疗的高剂量吸入和全身用类固醇有关。在服务结构和患者获得重度哮喘护理方面存在显著异质性,包括获得生物治疗的机会。似乎过度依赖短效β受体激动剂和频繁使用口服糖皮质激素,这两个未控制哮喘的指标可能表明存在未诊断或治疗不充分的重度哮喘。这个改良的德尔菲共识项目的目的是在证据不足的领域,通过患者和医疗保健专业人员的共识来定义加拿大重度哮喘的护理标准,以补充即将出台的指南。
哮喘专家指导小组确定了由八个关键主题形成的43条陈述。向加拿大各地从事哮喘工作的医疗保健专业人员发送了一份在线4级李克特量表问卷,以评估对这些陈述的认同(共识)。如果≥75%的受访者同意某一陈述,则定义为高共识;如果≥90%的受访者同意某一陈述,则定义为非常高的共识。
共收到150名医疗保健专业人员的回复,包括认证呼吸教育工作者、呼吸科医生、过敏症专科医生、全科医生/家庭医生、护士、药剂师和呼吸治疗师。受访者中,37条(86%)陈述达成了非常高的共识,4条(9%)陈述达成了高共识,2条(5%)陈述未达成共识。根据共识得分,提出了十条关键建议。这些建议侧重于初级和二级护理的转诊、获得专科哮喘服务、为重度哮喘患者提供家庭护理以及结果指标。
在加拿大重度哮喘护理路径中实施这些建议,有可能通过更早发现未诊断的重度哮喘、缩短重度哮喘诊断时间以及启动针对晚期表型的特异性治疗,改善患者的治疗结果。