AstraZeneca, Cambridge, United Kingdom.
AstraZeneca, Gaithersburg, Maryland.
Clin Cancer Res. 2023 Jun 1;29(11):2066-2074. doi: 10.1158/1078-0432.CCR-22-2765.
Biomarkers that predict response to immune checkpoint inhibitors (ICI) in recurrent or metastatic head and neck squamous cell carcinoma (R/M HNSCC) are needed. This retrospective study assessed tumor mutational burden (TMB) and outcomes in the phase II HAWK and CONDOR and phase III EAGLE studies of durvalumab with or without tremelimumab in platinum-resistant R/M HNSCC.
Tumor samples from HAWK/CONDOR (N = 153) and blood samples from EAGLE (N = 247) were analyzed for TMB. Associations with survival were evaluated for tissue TMB (tTMB) at cutoffs from 10 to 20 mutations/megabase (mut/Mb) and for blood plasma TMB (bTMB) at cutoffs from 8 to 24 mut/Mb.
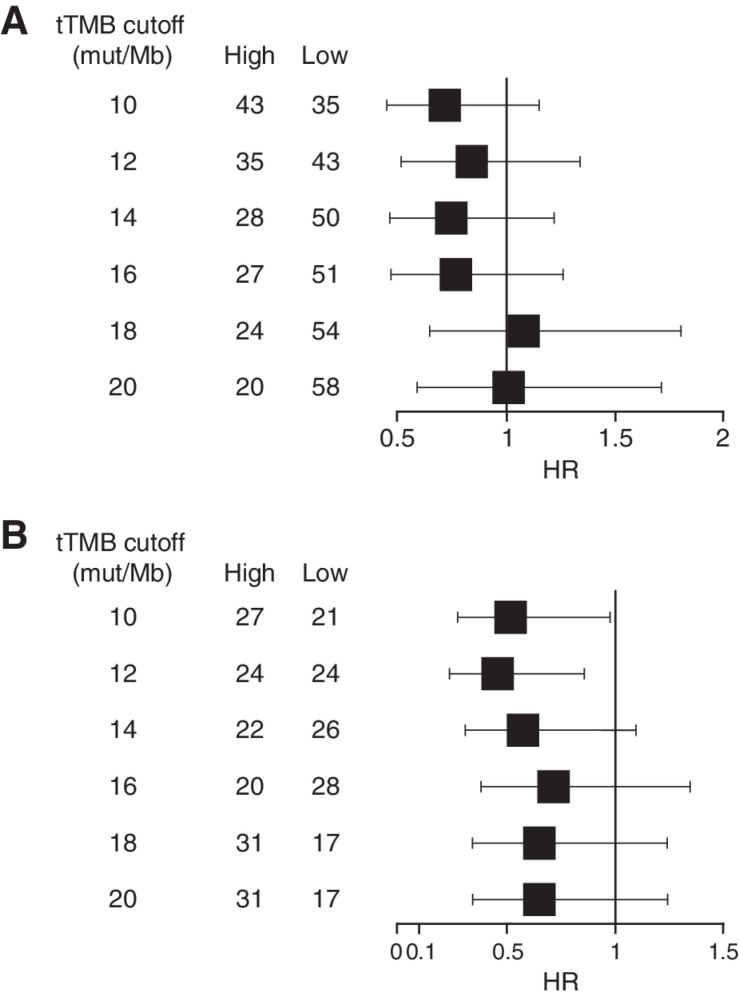
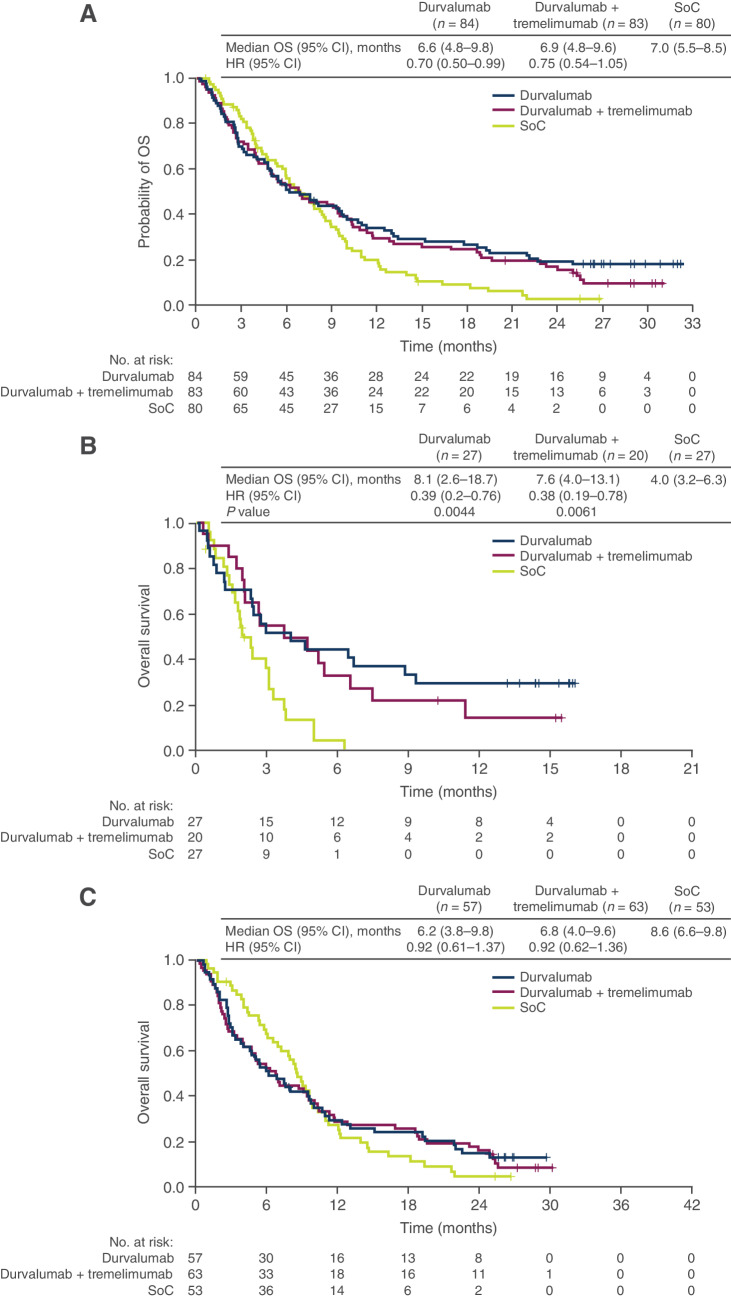
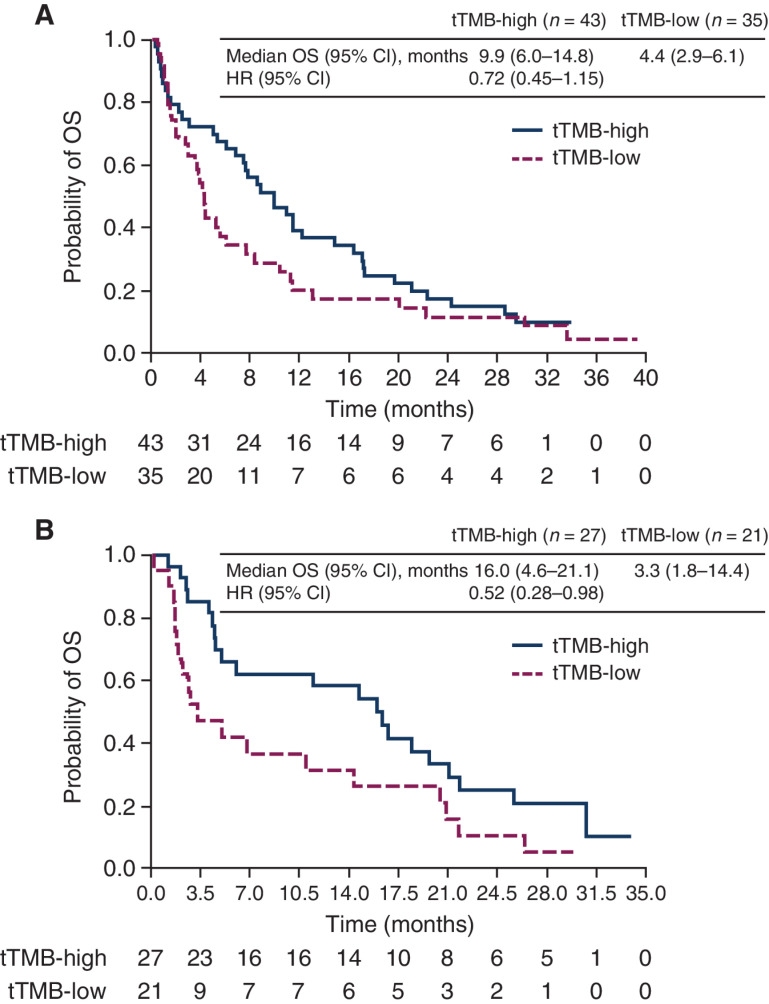
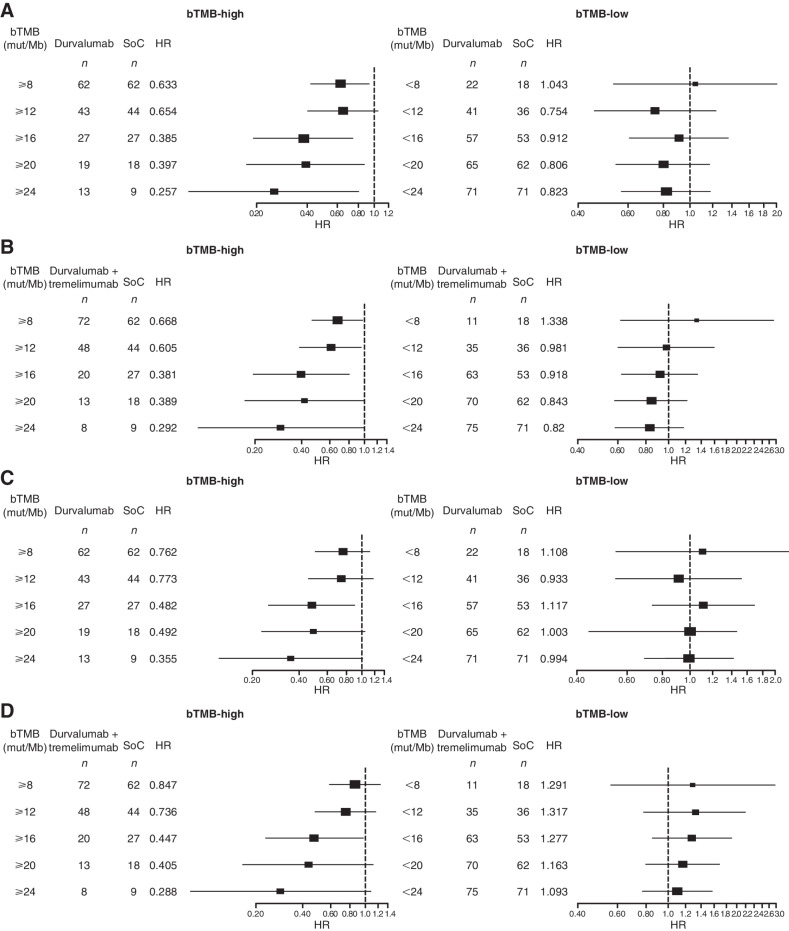
In HAWK/CONDOR, overall survival (OS) with durvalumab with or without tremelimumab was longer for high versus low tTMB: statistically significant differences were observed with durvalumab plus tremelimumab at tTMB ≥ 10 mut/Mb [HR, 0.52 (95% confidence interval, CI, 0.28-0.98)] and tTMB ≥ 12 mut/Mb [HR, 0.46 (95% CI, 0.24-0.86)]. In EAGLE, a significant OS benefit versus chemotherapy was observed with durvalumab and durvalumab plus tremelimumab at bTMB≥16 mut/Mb [HR, 0.39 (95% CI, 0.20-0.76) and 0.38 (95% CI, 0.19-0.78), respectively] but not bTMB < 16 mut/Mb [HR, 0.92 (0.61-1.37) and 0.92 (95% CI, 0.62-1.36), respectively]. A significant progression-free survival benefit was also observed in the ICI arms versus chemotherapy at bTMB ≥ 16 mut/Mb.
Findings support TMB as a biomarker for predicting survival in patients with platinum-resistant R/M HNSCC treated with ICIs. The analysis of EAGLE demonstrated that bTMB was predictive of survival with ICI treatment versus chemotherapy in a large, randomized controlled study population.
需要生物标志物来预测复发性或转移性头颈部鳞状细胞癌(R/M HNSCC)对免疫检查点抑制剂(ICI)的反应。这项回顾性研究评估了 durvalumab 联合或不联合 tremelimumab 治疗铂类耐药 R/M HNSCC 的 II 期 HAWK 和 CONDOR 以及 III 期 EAGLE 研究中的肿瘤突变负担(TMB)和结果。
分析了来自 HAWK/CONDOR(N=153)的肿瘤样本和来自 EAGLE(N=247)的血液样本,以评估 TMB。对于组织 TMB(tTMB),在 10 至 20 个突变/Mb(mut/Mb)的截止值和血液血浆 TMB(bTMB)在 8 至 24 mut/Mb 的截止值处评估与生存的相关性。
在 HAWK/CONDOR 中,durvalumab 联合或不联合 tremelimumab 的总生存期(OS)对于高 tTMB 与低 tTMB 较长:durvalumab 联合 tremelimumab 在 tTMB≥10 mut/Mb 时观察到具有统计学意义的差异[HR,0.52(95%置信区间,CI,0.28-0.98)]和 tTMB≥12 mut/Mb [HR,0.46(95%CI,0.24-0.86)]。在 EAGLE 中,与化疗相比,durvalumab 和 durvalumab 联合 tremelimumab 在 bTMB≥16 mut/Mb 时观察到显著的 OS 获益[HR,0.39(95%CI,0.20-0.76)和 0.38(95%CI,0.19-0.78)],但 bTMB<16 mut/Mb 时无显著获益[HR,0.92(0.61-1.37)和 0.92(95%CI,0.62-1.36)]。在 bTMB≥16 mut/Mb 时,ICI 臂与化疗相比,还观察到无进展生存期的显著获益。
研究结果支持 TMB 作为预测铂类耐药 R/M HNSCC 患者接受 ICI 治疗后生存的生物标志物。EAGLE 的分析表明,在一项大型随机对照研究人群中,bTMB 可预测 ICI 治疗与化疗的生存获益。