Department of Perinatology, Division of Obstetrics and Gynecology, University Medical Center Ljubljana, Ljubljana, Slovenia.
Department of Obstetrics and Gynecology, General Hospital Slovenj Gradec, Slovenj Gradec, Slovenia.
J Pregnancy. 2023 Feb 13;2023:5853889. doi: 10.1155/2023/5853889. eCollection 2023.
To compare diagnostic values of four intrapartum cardiotocography (CTG) classifications in predicting neonatal acidemia at birth.
Retrospective case-control study. Forty-three CTG traces with an umbilical artery pH < 7.00 (study group) and 43 traces with a pH ≥ 7.00 (control group) were analyzed. Inclusion criteria were singleton pregnancy, cephalic presentation, admission to labour ward during active phase of first stage of labour, and gestational age 37 to 41 weeks. Exclusion criteria were suspected intrauterine growth restriction, oligohydramnios, polyhydramnios, pregestational or gestational insulin-dependent diabetes mellitus, and preeclampsia. Last 30-60 minutes before delivery of CTG traces was classified retrospectively according to four classification systems-International Federation of Gynecology and Obstetrics (FIGO), Royal College of Obstetricians and Gynaecologists (RCOG), National Institute of Child Health and Human Development (NICHD), and the 5-tier system by Parer and Ikeda. Predictive value of each classification for neonatal acidemia was assessed using receiver operating characteristics (ROC) analysis.
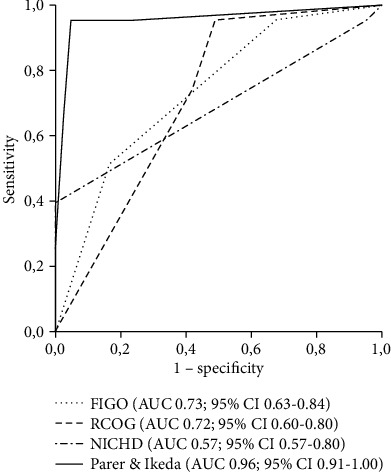
FIGO, RCOG, and NICHD classifications predicted neonatal acidemia with areas under the ROC curves (AUC) of 0.73, 95% confidence interval (CI) 0.63-0.84; 0.72, 95% CI 0.60-0.83; and 0.69, 95% CI 0.57-0.80, respectively. The five-tier system by Parer and Ikeda had significantly better predictive value with an AUC of 0.96, 95% CI 0.91-1.00.
The 5-tier classification system proposed by Parer and Ikeda for assessing CTG in labour was superior to FIGO, RCOG, and NICHD intrapartum CTG classifications in predicting severe neonatal acidemia at birth.
比较 4 种产时胎心监护(CTG)分类方法在预测出生时新生儿酸中毒中的诊断价值。
回顾性病例对照研究。分析 43 份脐动脉 pH 值<7.00 的 CTG 图(研究组)和 43 份 pH 值≥7.00 的 CTG 图(对照组)。纳入标准为单胎妊娠、头位、第一产程活跃期入院、孕龄 37 至 41 周。排除标准为可疑宫内生长受限、羊水过少、羊水过多、孕前或妊娠期胰岛素依赖型糖尿病、子痫前期。分娩前最后 30-60 分钟的 CTG 图按国际妇产科联合会(FIGO)、英国皇家妇产科医师学院(RCOG)、美国国立儿童健康与人类发育研究所(NICHD)和 Parer 和 Ikeda 的 5 级系统进行回顾性分类。使用受试者工作特征(ROC)曲线分析每种分类方法对新生儿酸中毒的预测价值。
FIGO、RCOG 和 NICHD 分类预测新生儿酸中毒的 ROC 曲线下面积(AUC)分别为 0.73、95%可信区间(CI)0.63-0.84;0.72、95% CI 0.60-0.83;0.69、95% CI 0.57-0.80。Parer 和 Ikeda 的 5 级系统具有更好的预测价值,AUC 为 0.96、95% CI 0.91-1.00。
Parer 和 Ikeda 提出的用于评估产时 CTG 的 5 级分类系统在预测出生时严重新生儿酸中毒方面优于 FIGO、RCOG 和 NICHD 产时 CTG 分类。