Halilu Fatima, Qureshi Anum, Nash Brenton
Greater Baltimore Medical Center, Towson, MD, USA.
J Community Hosp Intern Med Perspect. 2022 Nov 7;12(6):73-78. doi: 10.55729/2000-9666.1129. eCollection 2022.
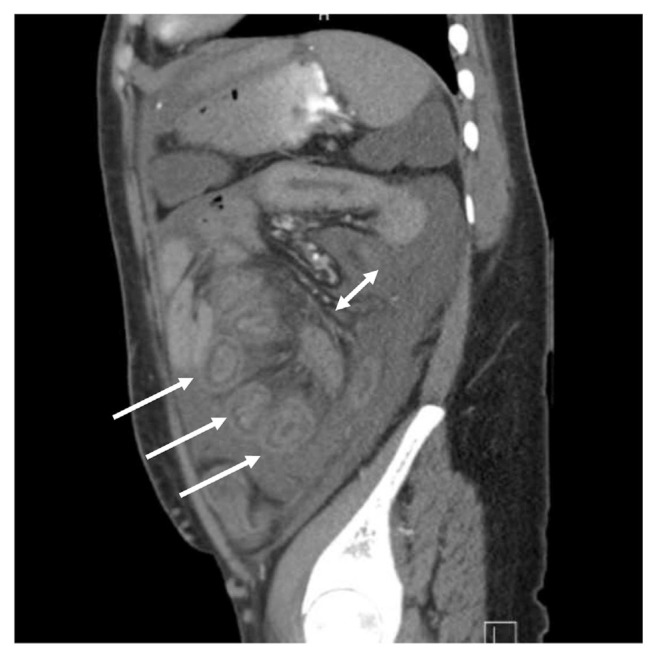
Lupus enteritis is a rare manifestation seen in systemic lupus erythematosus (SLE). Its diagnosis can be challenging as symptoms frequently overlap many gastrointestinal disorders, imaging findings are not specific, and endoscopic features are infrequently diagnostic. Moreover, enteritis can occur in isolation without other systemic manifestations or even elevated inflammatory markers.1 Here is presented the case of a 22-year-old female with known SLE manifested by lupus nephritis complicated by end-stage renal disease who presented with abdominal pain. She had leukocytosis with thickened bowel loops, ascites, "target sign", "comb sign" and patent abdominal vessels on CT imaging. The differential diagnoses considered ranged from infectious gastroenteritis to systemic vasculitis. Her infectious workup was negative while inflammatory markers and autoimmune workup did not support active lupus flare. Having ruled out alternative etiologies, steroid dosing was increased in consultation with rheumatology. Subsequently, her abdominal pain responded supporting a diagnosis of lupus enteritis. The case was perplexing in light of her non-specific presenting symptoms and the absence of laboratory evidence of active lupus flare which delayed the diagnosis. This case illustrates how the diagnosis of lupus enteritis continues to remain a challenge.
狼疮性肠炎是系统性红斑狼疮(SLE)中一种罕见的表现形式。其诊断具有挑战性,因为症状常常与许多胃肠道疾病重叠,影像学表现不具特异性,且内镜特征很少具有诊断价值。此外,肠炎可单独发生,无其他全身表现,甚至炎症标志物也不升高。1 本文介绍了一名 22 岁已知患有 SLE 的女性病例,该患者以狼疮性肾炎合并终末期肾病为表现,出现腹痛。她白细胞增多,CT 成像显示肠袢增厚、腹水、“靶征”、“梳征”及腹部血管通畅。考虑的鉴别诊断范围从感染性肠胃炎到系统性血管炎。她的感染检查结果为阴性,而炎症标志物和自身免疫检查结果不支持狼疮活动期发作。在排除其他病因后,与风湿病科会诊后增加了类固醇剂量。随后,她的腹痛症状有所缓解,支持狼疮性肠炎的诊断。鉴于她的非特异性症状以及缺乏狼疮活动期发作的实验室证据,该病例令人困惑,延迟了诊断。此病例说明了狼疮性肠炎的诊断仍然是一项挑战。