Vaccarella Salvatore, Georges Damien, Bray Freddie, Ginsburg Ophira, Charvat Hadrien, Martikainen Pekka, Brønnum-Hansen Henrik, Deboosere Patrick, Bopp Matthias, Leinsalu Mall, Artnik Barbara, Lorenzoni Valentina, De Vries Esther, Marmot Michael, Vineis Paolo, Mackenbach Johan, Nusselder Wilma
Cancer Surveillance Branch, International Agency for Research on Cancer (IARC/WHO), Lyon, France.
Early Detection, Prevention, and Infections Branch, International Agency for Research on Cancer (IARC/WHO), Lyon, France.
Lancet Reg Health Eur. 2022 Nov 28;25:100551. doi: 10.1016/j.lanepe.2022.100551. eCollection 2023 Feb.
Reducing socioeconomic inequalities in cancer is a priority for the public health agenda. A systematic assessment and benchmarking of socioeconomic inequalities in cancer across many countries and over time in Europe is not yet available.
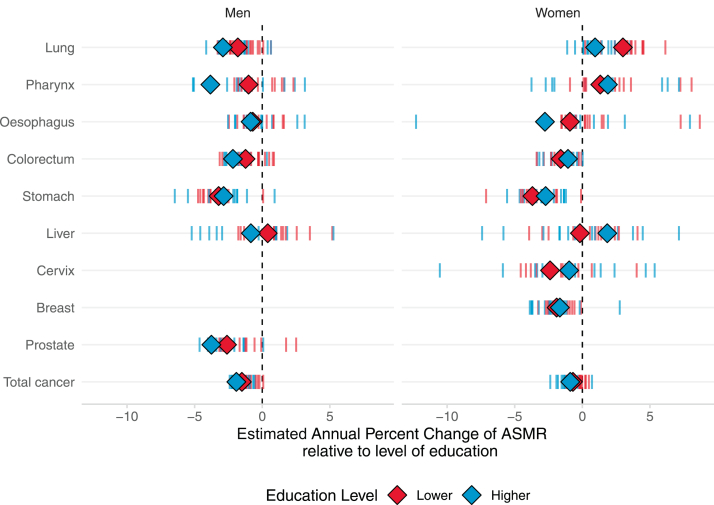
Census-linked, whole-of-population cancer-specific mortality data by socioeconomic position, as measured by education level, and sex were collected, harmonized, analysed, and compared across 18 countries during 1990-2015, in adults aged 40-79. We computed absolute and relative educational inequalities; temporal trends using estimated-annual-percentage-changes; the share of cancer mortality linked to educational inequalities.
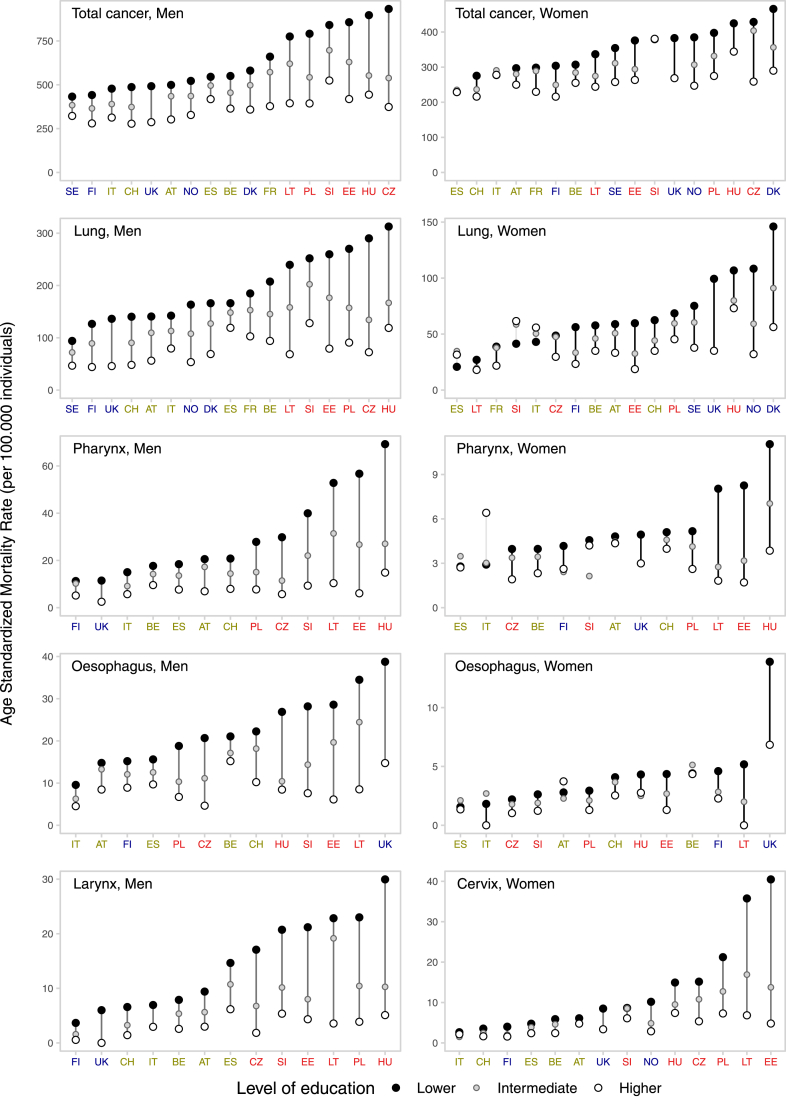
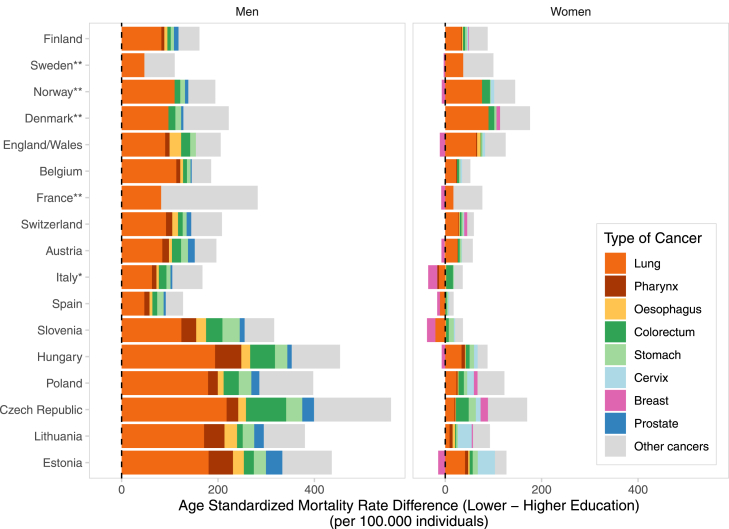
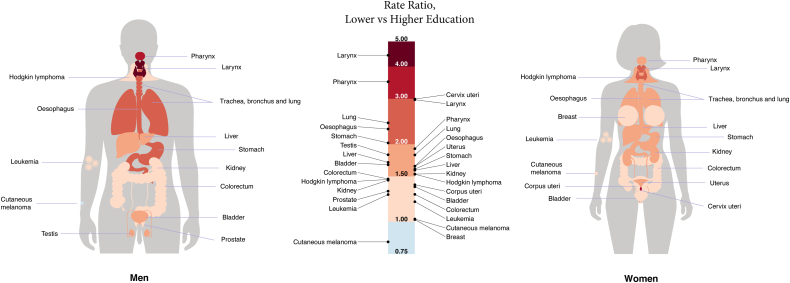
Everywhere in Europe, lower-educated individuals have higher mortality rates for nearly all cancer-types relative to their more highly-educated counterparts, particularly for tobacco/infection-related cancers [relative risk of lung cancer mortality for lower- versus higher-educated = 2.4 (95% confidence intervals: 2.1-2.8) among men; = 1.8 (95% confidence intervals: 1.5-2.1) among women]. However, the magnitude of inequalities varies greatly by country and over time, predominantly due to differences in cancer mortality among lower-educated groups, as for many cancer-types higher-educated have more similar (and lower) rates, irrespective of the country. Inequalities were generally greater in Baltic/Central/East-Europe and smaller in South-Europe, although among women large and rising inequalities were found in North-Europe (relative risk of all cancer mortality for lower- versus higher-educated ≥1.4 in Denmark, Norway, Sweden, Finland and the England/Wales). Among men, rate differences (per 100,000 person-years) in total-cancer mortality for lower-vs-higher-educated groups ranged from 110 (Sweden) to 559 (Czech Republic); among women from approximately null (Slovenia, Italy, Spain) to 176 (Denmark). Lung cancer was the largest contributor to inequalities in total-cancer mortality (between-country range: men, 29-61%; women, 10-56%). 32% of cancer deaths in men and 16% in women (but up to 46% and 24%, respectively in Baltic/Central/East-Europe) were associated with educational inequalities.
Cancer mortality in Europe is largely driven by levels and trends of cancer mortality rates in lower-education groups. Even Nordic-countries, with a long-established tradition of equitable welfare and social justice policies, witness increases in cancer inequalities among women. These results call for a systematic measurement, monitoring and action upon the remarkable socioeconomic inequalities in cancer existing in Europe.
This study was done as part of the LIFEPATH project, which has received financial support from the European Commission (Horizon 2020 grant number 633666), and the DEMETRIQ project, which received support from the European Commission (grant numbers FP7-CP-FP and 278511). SV and WN were supported by the French Institut National du Cancer (INCa) (Grant number 2018-116). PM was supported by the Academy of Finland (#308247, # 345219) and the European Research Council under the European Union's Horizon 2020 research and innovation programme (grant agreement No 101019329). The work by Mall Leinsalu was supported by the Estonian Research Council (grant PRG722).
减少癌症方面的社会经济不平等是公共卫生议程的一项优先事项。目前尚无对欧洲多个国家长期以来癌症社会经济不平等状况的系统评估和基准设定。
收集了1990 - 2015年期间18个国家40 - 79岁成年人按教育水平衡量的社会经济地位和性别的与人口普查相关的全人群特定癌症死亡率数据,进行了统一、分析和比较。我们计算了绝对和相对教育不平等;使用估计的年百分比变化计算时间趋势;计算与教育不平等相关的癌症死亡率占比。
在欧洲各地,受教育程度较低的个体几乎在所有癌症类型上的死亡率都高于受教育程度较高的个体,尤其是在烟草/感染相关癌症方面[男性中,受教育程度较低与较高者肺癌死亡率的相对风险 = 2.4(95%置信区间:2.1 - 2.8);女性中 = 1.8(95%置信区间:1.5 - 2.1)]。然而,不平等的程度因国家和时间差异很大,主要是由于受教育程度较低群体中癌症死亡率的差异,因为对于许多癌症类型,无论哪个国家,受教育程度较高者的死亡率更为相似(且较低)。波罗的海/中欧/东欧的不平等通常更大,南欧的不平等较小,不过在北欧,女性中发现不平等现象大且在增加(丹麦、挪威、瑞典、芬兰以及英格兰/威尔士中,受教育程度较低与较高者所有癌症死亡率的相对风险≥1.4)。在男性中,受教育程度较低与较高群体每10万人年的总癌症死亡率差异范围为110(瑞典)至559(捷克共和国);在女性中,差异范围从几乎为零(斯洛文尼亚、意大利、西班牙)至176(丹麦)。肺癌是总癌症死亡率不平等的最大促成因素(国家间范围:男性为29% - 61%;女性为10% - 56%)。男性中32%的癌症死亡和女性中16%的癌症死亡(但在波罗的海/中欧/东欧分别高达46%和24%)与教育不平等相关。
欧洲的癌症死亡率在很大程度上由受教育程度较低群体的癌症死亡率水平和趋势所驱动。即使是有着长期公平福利和社会正义政策传统的北欧国家,女性中的癌症不平等现象也在增加。这些结果呼吁对欧洲存在的显著癌症社会经济不平等进行系统的测量、监测和采取行动。
本研究是作为LIFEPATH项目(该项目获得了欧盟委员会的资金支持,地平线2020资助编号633666)以及DEMETRIQ项目(该项目获得了欧盟委员会的支持,资助编号FP7 - CP - FP和278511)的一部分完成的。SV和WN得到了法国国家癌症研究所(INCa)的支持(资助编号2018 - 116)。PM得到了芬兰科学院(#308247,#345219)以及欧盟地平线2020研究与创新计划下的欧洲研究理事会的支持(资助协议编号101019329)。Mall Leinsalu的工作得到了爱沙尼亚研究理事会(资助编号PRG722)的支持。