Department of Orthopedic Surgery, The First Hospital of Hebei Medical University, Shijiazhuang, Hebei, PR China.
Lingshui Hospital of First Hospital of Hebei Medical University, Lingshui, Hainan, PR China.
Medicine (Baltimore). 2023 Feb 10;102(6):e32941. doi: 10.1097/MD.0000000000032941.
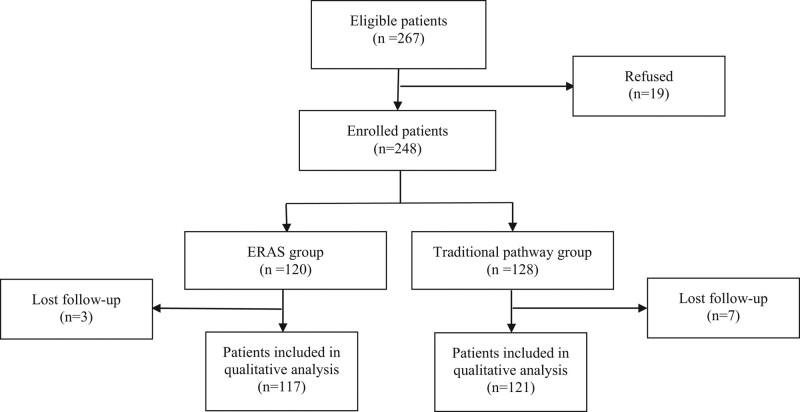
The enhanced recovery after surgery (ERAS) pathway was formulated with the aim to reduce surgical stress response, alleviate pain and guarantee the best-fit experience of patients' perioperative period. However, the application of ERAS in geriatric patients who underwent unicompartmental knee arthroplasty (UKA) was relatively lacking. We hypothesize that UKA patients can benefit from the ERAS protocol. A total of 238 patients were recruited in this retrospective study from August 2018 to December 2021, and Oxford phase III UKA was applied to all patients. ERAS pathway included nutrition support, anesthesia mode, interoperative temperature, and blood pressure control, application of tranexamic acid, early initiation of oral intake and mobilization, and pain management. Demographic data, operation-relative variables, and postoperative complications were analyzed. Forgotten Joint Scores, Oxford Knee Score, Lysholm score, numerical rating scale, and knee range of motion were introduced to estimate the activity function and pain of surgical knee, and these variables were compared between the 2 groups. There were 117 patients in the ERAS group and 121 patients in the traditional group, respectively. The ERAS group had a shorter length of surgical incision and less intraoperative blood loss. Postoperative hemoglobin and albumin of patients in the ERAS group were better than those in the traditional group (P < .05), after 17.0 ± 10.8 months follow-up, the numerical rating scale, Lysholm, Oxford Knee Score, Forgotten Joint Scores, and knee range of motion of patients in the ERAS group were significantly better than the traditional group. The length of hospital stay for patients who underwent ERAS was 11.7 ± 3.8 days and the postoperative complication rate was lower for the ERAS group patients (P = .000 and 0.031). ERAS can reduce the length of hospital stay, and patients can achieve excellent postoperative knee function. The formulation and implementation of the ERAS protocol require good collaboration across multiple disciplines, as well as a deep understanding of the existing clinical evidence and the concept of the ERAS program.
术后加速康复(ERAS)途径的制定旨在减轻手术应激反应,缓解疼痛,并确保患者围手术期的最佳体验。然而,在接受单髁膝关节置换术(UKA)的老年患者中,ERAS 的应用相对较少。我们假设 UKA 患者可以从 ERAS 方案中受益。本回顾性研究共纳入 2018 年 8 月至 2021 年 12 月的 238 例患者,所有患者均接受牛津 III 期 UKA。ERAS 途径包括营养支持、麻醉方式、术中体温和血压控制、氨甲环酸的应用、早期口服和活动、疼痛管理。分析了人口统计学数据、手术相关变量和术后并发症。采用遗忘关节评分、牛津膝关节评分、Lysholm 评分、数字评分量表和膝关节活动范围来评估手术膝关节的活动功能和疼痛,并比较两组间的差异。ERAS 组 117 例,传统组 121 例。ERAS 组的手术切口较短,术中失血量较少。ERAS 组患者术后血红蛋白和白蛋白优于传统组(P<0.05),随访 17.0±10.8 个月后,ERAS 组患者的数字评分量表、Lysholm、牛津膝关节评分、遗忘关节评分和膝关节活动度明显优于传统组。ERAS 组患者的住院时间为 11.7±3.8 天,术后并发症发生率较低(P=0.000 和 0.031)。ERAS 可缩短住院时间,使患者获得良好的术后膝关节功能。ERAS 方案的制定和实施需要多学科之间的良好合作,以及对现有临床证据和 ERAS 方案理念的深入理解。