Zang Lianru, Gu Kaihao, Ji Xingkai, Zhang Hao, Yan Shengjie, Wu Xiaomei
Center for Biomedical Engineering, School of Information Science and Technology, Fudan University, Shanghai 200438, China.
Academy for Engineering and Technology, Fudan University, Shanghai 200433, China.
J Cardiovasc Dev Dis. 2023 Jan 30;10(2):56. doi: 10.3390/jcdd10020056.
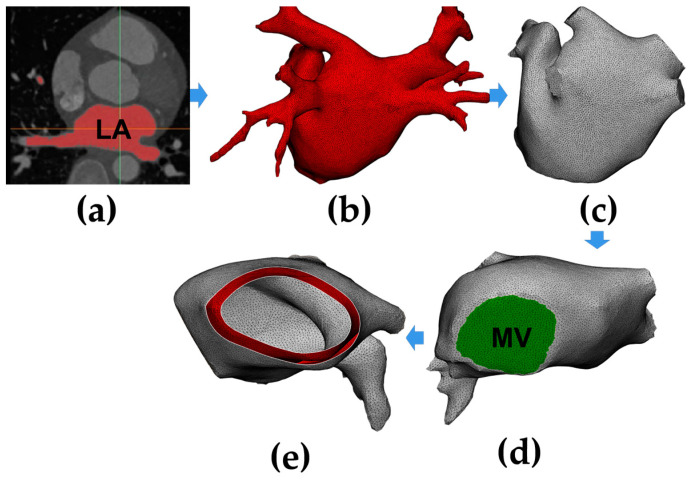
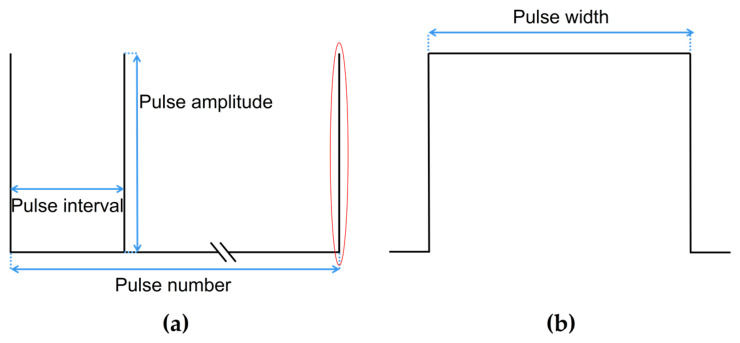
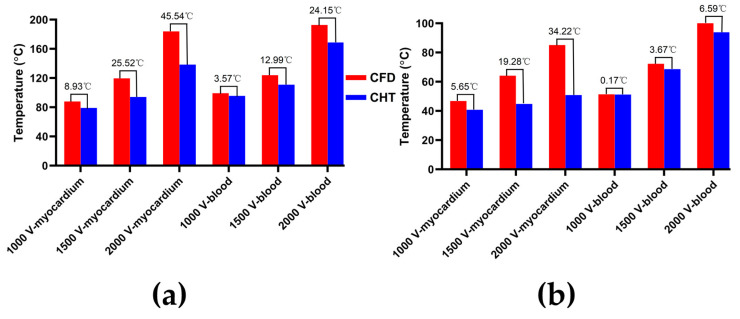
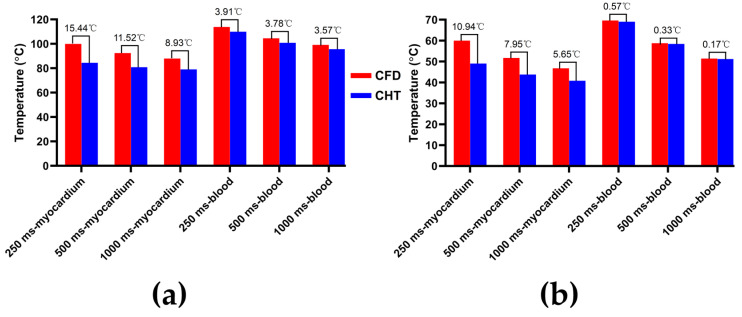
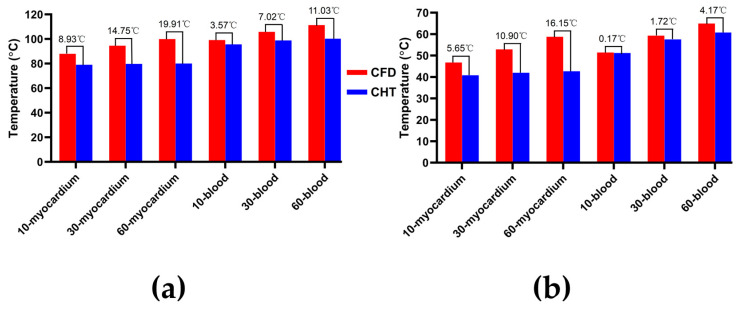
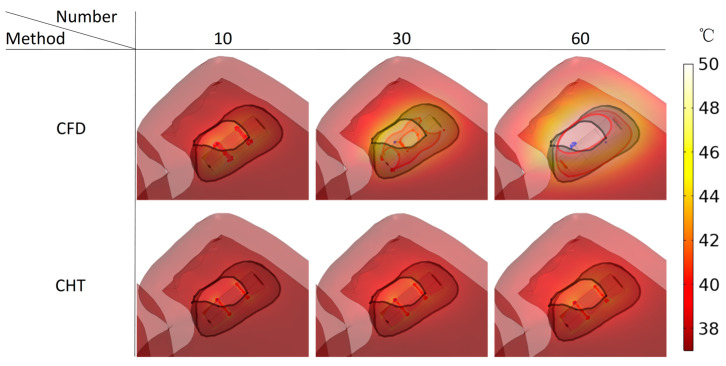
The non-thermal effects are considered one of the prominent advantages of pulsed field ablation (PFA). However, at higher PFA doses, the temperature rise in the tissue during PFA may exceed the thermal damage threshold, at which time intracardiac pulsatile blood flow plays a crucial role in suppressing this temperature rise. This study aims to compare the effect of heat dissipation of the different methods in simulating the pulsatile blood flow during PFA. This study first constructed an anatomy-based left atrium (LA) model and then applied the convective heat transfer (CHT) method and the computational fluid dynamics (CFD) method to the model, respectively, and the thermal convective coefficients used in the CHT method are 984 (W/mK) (blood-myocardium interface) and 4372 (W/mK) (blood-catheter interface), respectively. Then, it compared the effect of the above two methods on the maximum temperature of myocardium and blood, as well as the myocardial ablation volumes caused by irreversible electroporation (IRE) and hyperthermia under different PFA parameters. Compared with the CFD method, the CHT method underestimates the maximum temperature of myocardium and blood; the differences in the maximum temperature of myocardium and blood between the two methods at the end of the last pulse are significant (>1 °C), and the differences in the maximum temperature of blood at the end of the last pulse interval are significant (>1 °C) only at a pulse amplitude greater than 1000 V or pulse number greater than 10. Under the same pulse amplitude and different heat dissipation methods, the IRE ablation volumes are the same. Compared with the CFD method, the CHT method underestimates the hyperthermia ablation volume; the differences in the hyperthermia ablation volume are significant (>1 mm) only at a pulse amplitude greater than 1000 V, a pulse interval of 250 ms, or a pulse number greater than 10. Additionally, the hyperthermia ablation isosurfaces are completely wrapped by the IRE ablation isosurfaces in the myocardium. Thus, during PFA, compared with the CFD method, the CHT method cannot accurately simulate the maximum myocardial temperature; however, except at the above PFA parameters, the CHT method can accurately simulate the maximum blood temperature and the myocardial ablation volume caused by IRE and hyperthermia. Additionally, within the range of the PFA parameters used in this study, the temperature rise during PFA may not lead to the appearance of additional hyperthermia ablation areas beyond the IRE ablation area in the myocardium.
非热效应被认为是脉冲场消融(PFA)的突出优势之一。然而,在较高的PFA剂量下,PFA过程中组织内的温度升高可能超过热损伤阈值,此时心内搏动血流在抑制这种温度升高方面起着关键作用。本研究旨在比较不同方法在模拟PFA期间搏动血流时的散热效果。本研究首先构建了基于解剖结构的左心房(LA)模型,然后分别将对流换热(CHT)方法和计算流体动力学(CFD)方法应用于该模型,CHT方法中使用的热对流系数分别为984(W/mK)(血液 - 心肌界面)和4372(W/mK)(血液 - 导管界面)。然后,比较了上述两种方法对心肌和血液最高温度的影响,以及在不同PFA参数下不可逆电穿孔(IRE)和热疗引起的心肌消融体积。与CFD方法相比,CHT方法低估了心肌和血液的最高温度;在最后一个脉冲结束时,两种方法在心肌和血液最高温度上的差异显著(>1°C),并且仅在脉冲幅度大于1000 V或脉冲数大于10时,在最后一个脉冲间隔结束时血液最高温度的差异才显著(>1°C)。在相同的脉冲幅度和不同的散热方法下,IRE消融体积相同。与CFD方法相比,CHT方法低估了热疗消融体积;仅在脉冲幅度大于1000 V、脉冲间隔为250 ms或脉冲数大于10时,热疗消融体积的差异才显著(>1 mm)。此外,在心肌中,热疗消融等值面完全被IRE消融等值面包裹。因此,在PFA期间,与CFD方法相比,CHT方法不能准确模拟心肌的最高温度;然而,除了上述PFA参数外,CHT方法可以准确模拟最高血液温度以及IRE和热疗引起的心肌消融体积。此外,在本研究使用的PFA参数范围内,PFA期间的温度升高可能不会导致心肌中出现超出IRE消融区域的额外热疗消融区域。