Leukemia Service, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY.
Cell Therapy Service, Department of Medicine, Memorial Sloan Kettering Cancer Center, New York, NY.
Blood Adv. 2023 Jul 11;7(13):3087-3098. doi: 10.1182/bloodadvances.2022009212.
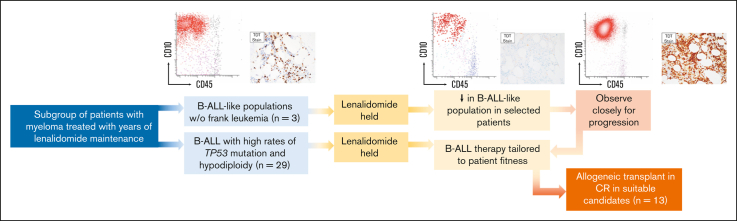
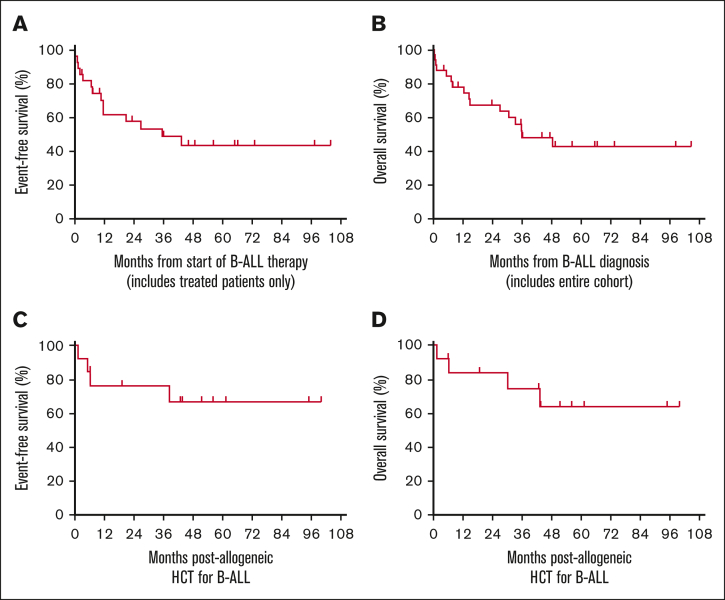
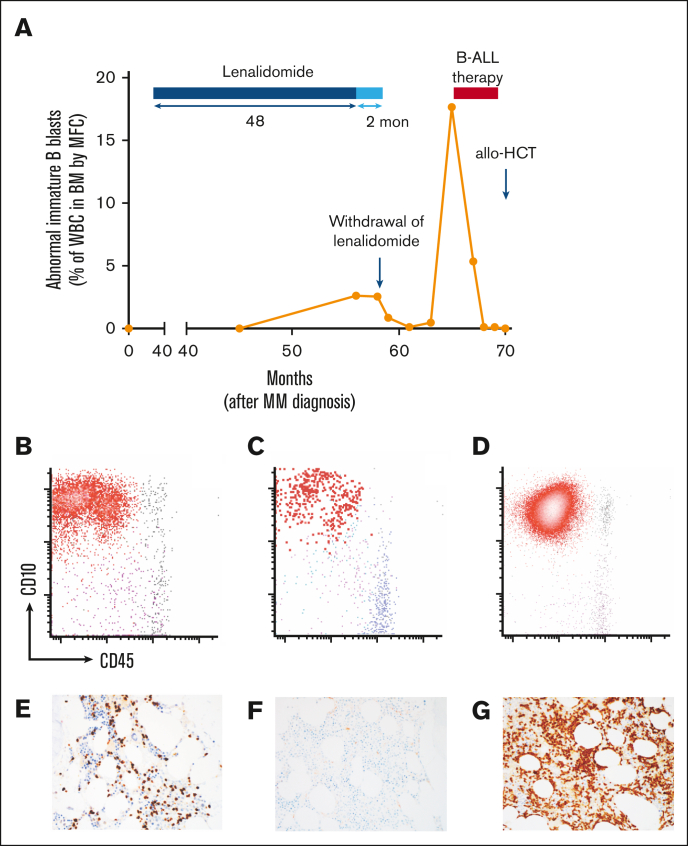
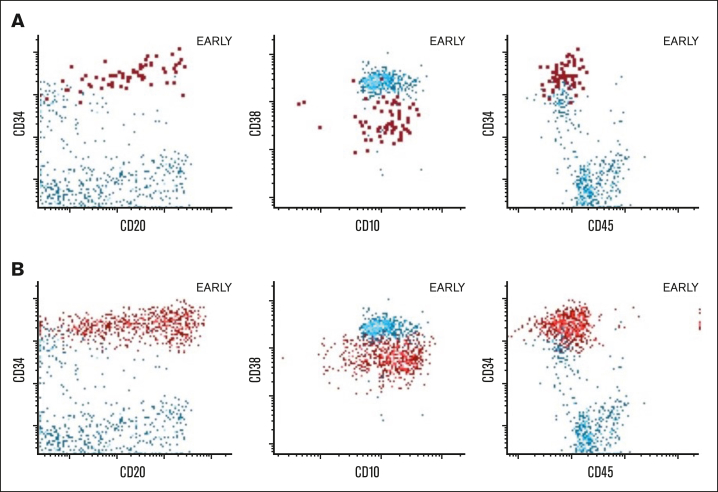
Lenalidomide is an effective component of induction and maintenance therapy for multiple myeloma, though with a risk of secondary malignancies, including acute lymphoblastic leukemia (ALL). In contrast to therapy-related myeloid neoplasia, lenalidomide-associated lymphoblastic neoplasia remains poorly characterized. We conducted a dual institution retrospective study of 32 ALL cases that arose after lenalidomide maintenance (all B-lineage, 31/32 BCR::ABL-negative). B-cell ALL (B-ALL) was diagnosed at median 54 months (range, 5-119) after first exposure to lenalidomide and after median 42 months of cumulative lenalidomide exposure (range, 2-114). High incidence of TP53 mutations (9/19 evaluable cases) and low hypodiploidy (8/26 patients) were identified. Despite median age of 65 years and poor-risk B-ALL features observed in the cohort, rates of complete response (CR) or CR with incomplete hematologic recovery were high (25/28 patients receiving treatment). Median event-free survival was 35.4 months among treated patients (not reached among those undergoing allogeneic hematopoietic cell transplantation [HCT]). Sixteen patients remain alive without evidence of B-ALL after HCT or extended maintenance therapy. We also describe regression of B-ALL or immature B-cell populations with B-ALL immunophenotype after lenalidomide discontinuation in 5 patients, suggesting lenalidomide may drive leukemic progression even after initiation of lymphoblastic neoplasia and that lenalidomide withdrawal alone may be an appropriate first-line intervention in selected patients. Monitoring for early B-ALL-like proliferations may offer opportunities for lenalidomide withdrawal to prevent progression. Established combination chemotherapy regimens, newer surface antigen-targeted approaches, and allogeneic HCT are effective in many patients with lenalidomide-associated B-ALL and should be offered to medically fit patients.
来那度胺是多发性骨髓瘤诱导和维持治疗的有效药物,但有发生继发性恶性肿瘤的风险,包括急性淋巴细胞白血病(ALL)。与治疗相关性髓系肿瘤不同,来那度胺相关的淋巴母细胞肿瘤的特征仍不清楚。我们对 32 例接受来那度胺维持治疗后发生的 ALL 病例进行了一项双机构回顾性研究(均为 B 细胞系,31/32 BCR::ABL 阴性)。B 细胞 ALL(B-ALL)在首次接触来那度胺后中位时间 54 个月(范围 5-119)时诊断,中位累积来那度胺暴露时间 42 个月(范围 2-114)。发现 9/19 例可评估病例中有高发生率的 TP53 突变和低低二倍体性(26 例患者中有 8 例)。尽管该队列中观察到中位年龄为 65 岁和高危 B-ALL 特征,但完全缓解(CR)或不完全血液学恢复的 CR 率较高(28 例接受治疗的患者中有 25 例)。治疗患者的中位无事件生存时间为 35.4 个月(接受异基因造血细胞移植[HCT]的患者未达到)。16 例患者在 HCT 或延长维持治疗后无 B-ALL 存活且无证据。我们还描述了在 5 例患者中断来那度胺后,B-ALL 或具有 B-ALL 免疫表型的不成熟 B 细胞群消退,表明即使在发生淋巴母细胞肿瘤后,来那度胺仍可能驱动白血病进展,单独停药可能是某些患者的合适一线干预措施。监测早期 B-ALL 样增殖可能为来那度胺停药以防止进展提供机会。许多接受来那度胺相关 B-ALL 治疗的患者对既定联合化疗方案、新型表面抗原靶向治疗和异基因 HCT 有效,应向符合条件的患者提供这些治疗。