Department of Orthopaedics, Trauma and Reconstructive Surgery, University Hospital RWTH Aachen, Pauwelsstraße 30, 52074, Aachen, Germany.
Department of Trauma, Hand, and Orthopaedic Surgery, Helios Dr. Horst Schmidt Kliniken Wiesbaden, Ludwig-Erhard-Straße 100, 65199, Wiesbaden, Germany.
Sci Rep. 2023 Feb 24;13(1):3260. doi: 10.1038/s41598-023-30461-x.
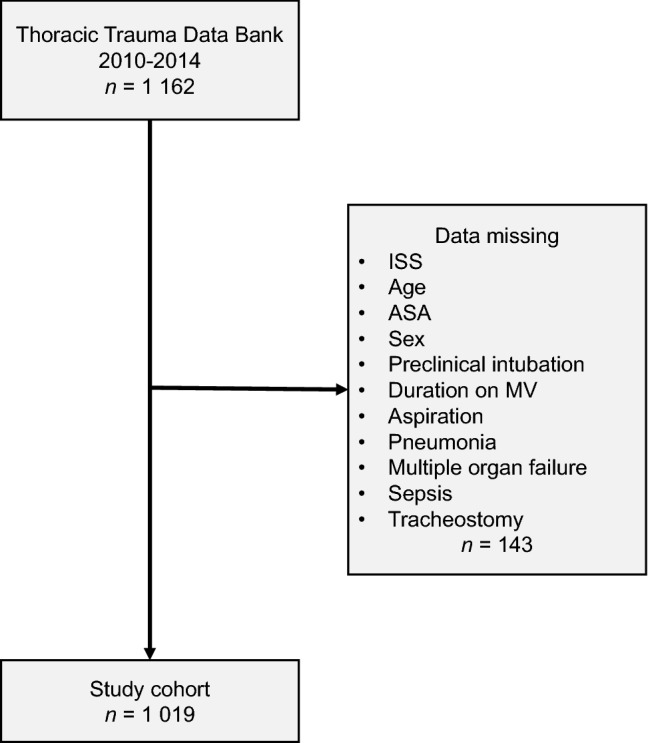
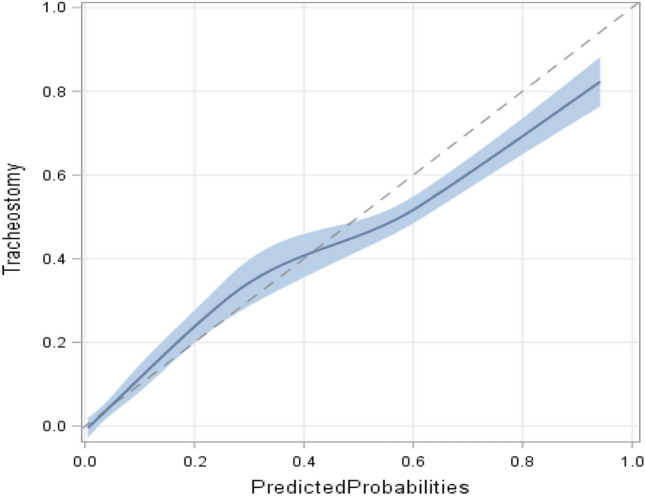
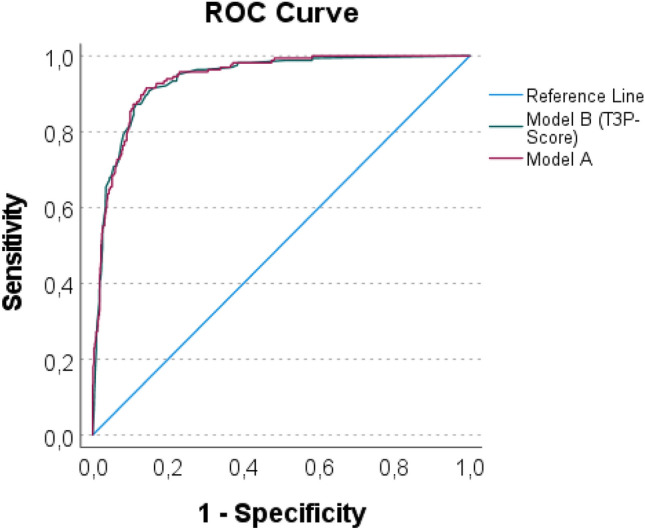
Multiple trauma patients with severe chest trauma are at increased risk for tracheostomy. While the risk factors associated with the need for tracheostomy are well established in the general critical care population, they have not yet been validated in a cohort of patients suffering severe thoracic trauma. This retrospective cohort study analysed data on patients aged 18 years or older who were admitted to one of the six participating academic level I trauma centres with multiple injuries, including severe thoracic trauma (AIS ≥ 3) between 2010 and 2014. A multivariable binary regression was used to identify predictor variables for tracheostomy and to develop the Tracheostomy in Thoracic Trauma Prediction Score (TP-Score). The study included 1019 adult thoracic trauma patients, of whom 165 underwent tracheostomy during their intensive care unit (ICU) stay. Prehospital endotracheal intubation (adjusted OR [AOR]: 2.494, 95% CI [1.412; 4.405]), diagnosis of pneumonia during the ICU stay (AOR: 4.374, 95% CI [2.503; 7.642]), duration of mechanical ventilation (AOR: 1.008/hours of intubation, 95% CI [1.006; 1.009]), and an AIS ≥ 3 (AOR 1.840, 95% CI [1.039; 3.261]) were independent risk factors for tracheostomy. Patients with sepsis had a lower risk of tracheostomy than patients without sepsis (AOR 0.486, 95% CI [0.253; 0.935]). The TP-Score had high predictive validity for tracheostomy (ROC = 0.938, 95% CI [0.920, 0.956]; Nagelkerke's R was 0.601). The TP-Score's specificity was 0.68, and the sensitivity was 0.96. The severity of thoracic trauma did not predict the need for tracheostomy. Follow-up studies should validate the TP-Score in external data sets and study the reasons for the reluctant use of tracheostomy in patients with severe thoracic trauma and subsequent sepsis.Trial registration: The study was applied for and registered a priori with the respective ethics committees.
多发伤合并严重胸部创伤的患者行气管切开术的风险增加。虽然在一般重症监护人群中,与气管切开术相关的危险因素已经得到很好的确立,但这些因素尚未在严重胸部创伤患者的队列中得到验证。这项回顾性队列研究分析了 2010 年至 2014 年期间,在六个参与的一级创伤中心之一因多发伤(包括严重胸部创伤 [AIS≥3])而入院的 18 岁或以上的患者的数据。使用多变量二项回归来确定气管切开术的预测变量,并制定胸外伤气管切开预测评分(TP-Score)。该研究纳入了 1019 例成人胸部创伤患者,其中 165 例在重症监护病房(ICU)期间行气管切开术。院外气管内插管(校正比值比 [AOR]:2.494,95%可信区间 [1.412; 4.405])、ICU 期间肺炎诊断(AOR:4.374,95%可信区间 [2.503; 7.642])、机械通气时间(AOR:1.008/小时插管,95%可信区间 [1.006; 1.009])和 AIS≥3(AOR 1.840,95%可信区间 [1.039; 3.261])是气管切开术的独立危险因素。脓毒症患者行气管切开术的风险低于非脓毒症患者(AOR 0.486,95%可信区间 [0.253; 0.935])。TP-Score 对气管切开术具有较高的预测价值(ROC=0.938,95%可信区间 [0.920,0.956];Nagelkerke 的 R 为 0.601)。TP-Score 的特异性为 0.68,敏感性为 0.96。胸部创伤的严重程度不能预测气管切开术的需要。后续研究应在外部数据集验证 TP-Score,并研究在严重胸部创伤和随后发生脓毒症的患者中不愿使用气管切开术的原因。
该研究已向相应的伦理委员会预先申请并注册。