Adegbite Bayode R, Edoa Jean R, Ndzebe Ndoumba Wilfrid F, Dimessa Mbadinga Lia B, Mombo-Ngoma Ghyslain, Jacob Shevin T, Rylance Jamie, Hänscheid Thomas, Adegnika Ayola A, Grobusch Martin P
Centre de Recherches Médicales de Lambaréné and African Partner Institution, German Center for Infection Research (CERMEL), Lambaréné, Gabon.
Center of Tropical Medicine and Travel Medicine, Department of Infectious Diseases, Amsterdam University Medical Centers, location AMC, Amsterdam Infection & Immunity, Amsterdam Public Health, University of Amsterdam, Amsterdam, The Netherlands.
EClinicalMedicine. 2021 Oct 30;42:101184. doi: 10.1016/j.eclinm.2021.101184. eCollection 2021 Dec.
Clinical scores for sepsis have been primarily developed for, and applied in High-Income Countries. This systematic review and meta-analysis examined the performance of the quick Sequential Organ Failure Assessment (qSOFA), Systemic Inflammatory Response Syndrome (SIRS), Modified Early Warning Score (MEWS), and Universal Vital Assessment (UVA) scores for diagnosis and prediction of mortality in patients with suspected infection in Low-and-Middle-Income Countries.
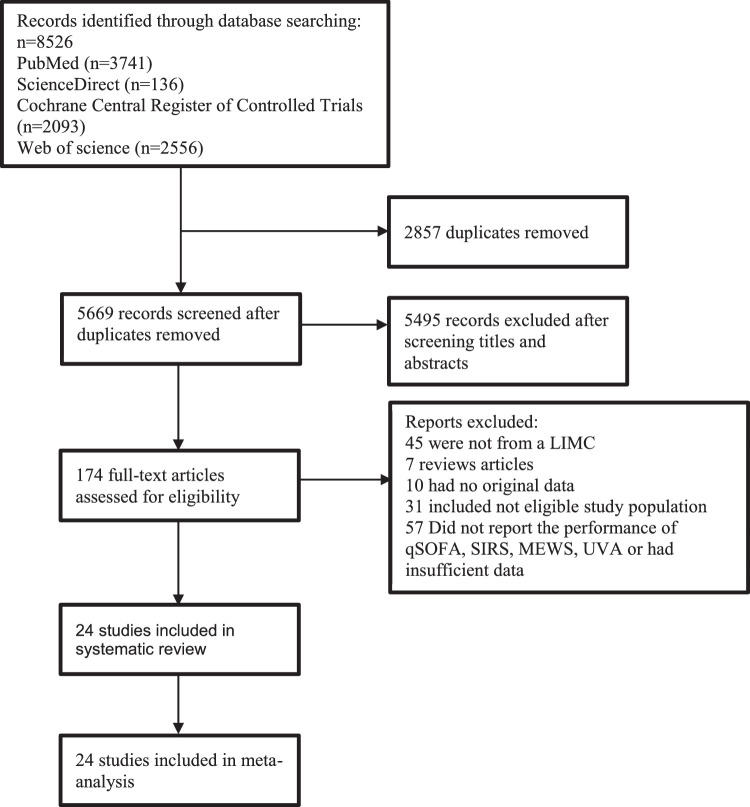
PubMed, Science Direct, Web of Science, and the Cochrane Central Register of Controlled Trials databases were searched until May 18, 2021. Studies reporting the performance of at least one of the above-mentioned scores for predicting mortality in patients of 15 years of age and older with suspected infection or sepsis were eligible. The Quality Assessment of Diagnostic Accuracy Studies tool was used for risk-of-bias assessment. PRISMA guidelines were followed (PROSPERO registration: CRD42020153906). The bivariate random-effects regression model was used to pool the individual sensitivities, specificities and areas-under-the-curve (AUC).
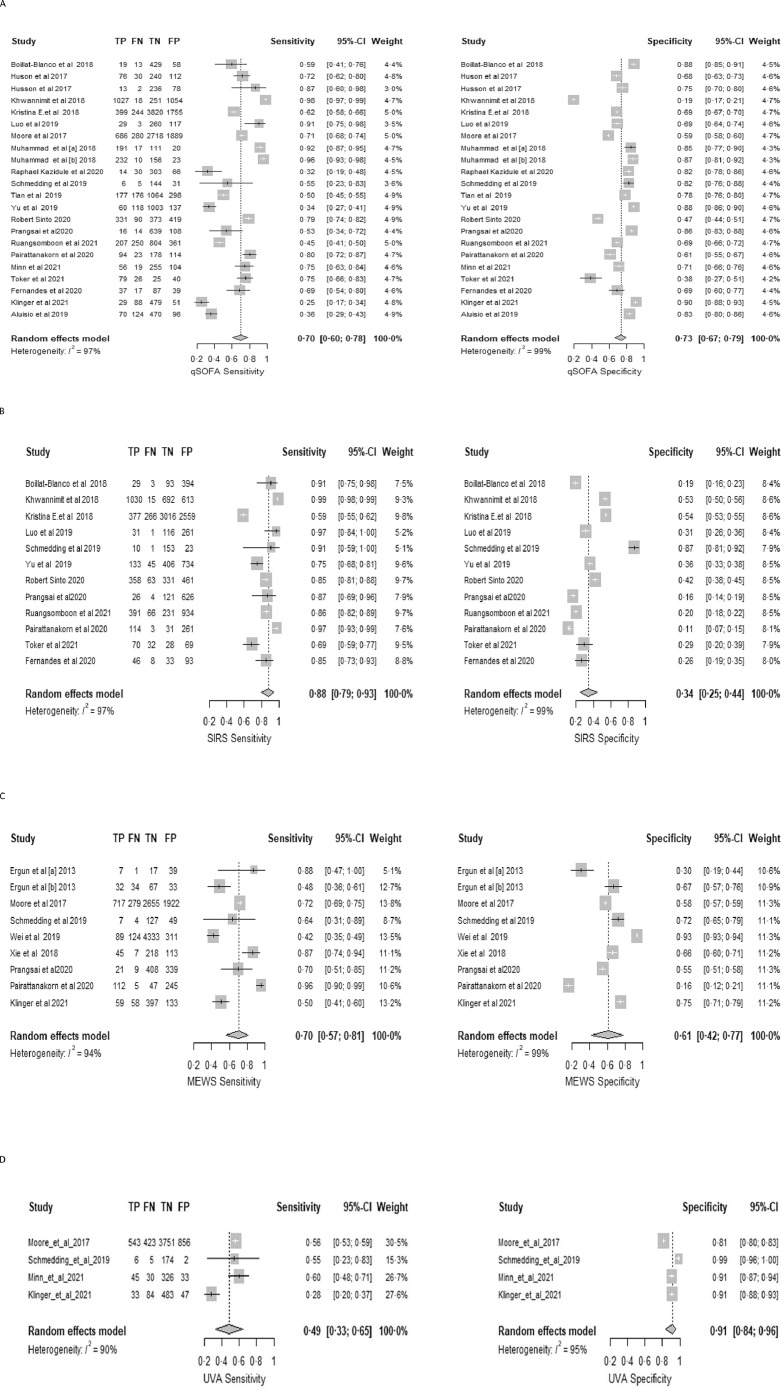
Twenty-four articles (of 5669 identified) with 27,237 patients were eligible for inclusion. qSOFA pooled sensitivity was 0·70 (95% confidence interval [CI] 0·60-0·78), specificity 0·73 (95% CI 0·67-0·79), and AUC 0·77 (95% CI 0·72-0·82). SIRS pooled sensitivity, specificity and AUC were 0·88 (95% CI 0·79 -0·93), 0·34 (95% CI 0·25-0·44), and 0·69 (95% CI 0·50-0·83), respectively. MEWS pooled sensitivity, specificity and AUC were 0·70 (95% CI 0·57 -0·81), 0·61 (95% CI 0·42-0·77), and 0·72 (95% CI 0·64-0·77), respectively. UVA pooled sensitivity, specificity and AUC were 0·49 (95% CI 0·33 -0·65), 0·91(95% CI 0·84-0·96), and 0·76 (95% CI 0·44-0·93), respectively. Significant heterogeneity was observed in the pooled analysis.
Individual score performances ranged from poor to acceptable. Future studies should combine selected or modified elements of different scores.
Partially funded by the UK National Institute for Health Research (NIHR) (17/63/42).
脓毒症临床评分主要是为高收入国家开发并应用于这些国家。本系统评价和荟萃分析研究了快速序贯器官衰竭评估(qSOFA)、全身炎症反应综合征(SIRS)、改良早期预警评分(MEWS)和通用生命体征评估(UVA)评分在低收入和中等收入国家疑似感染患者诊断及死亡预测中的表现。
检索了PubMed、Science Direct、Web of Science以及Cochrane对照试验中央注册库数据库,检索截止至2021年5月18日。纳入报告上述至少一种评分在15岁及以上疑似感染或脓毒症患者中预测死亡表现的研究。使用诊断准确性研究的质量评估工具进行偏倚风险评估。遵循PRISMA指南(PROSPERO注册号:CRD42020153906)。采用双变量随机效应回归模型汇总个体敏感性、特异性和曲线下面积(AUC)。
在检索到的5669篇文章中,有24篇文章纳入了27237例患者。qSOFA汇总敏感性为0.70(95%置信区间[CI]0.60 - 0.78),特异性为0.73(95%CI 0.67 - 0.79),AUC为0.77(95%CI 0.72 - 0.82)。SIRS汇总敏感性、特异性和AUC分别为0.88(95%CI 0.79 - 0.93)、0.34(95%CI 0.25 - 0.44)和0.69(95%CI 0.50 - 0.83)。MEWS汇总敏感性、特异性和AUC分别为0.70(95%CI 0.57 - 0.81)、0.61(95%CI 0.42 - 0.77)和0.72(95%CI 0.64 - 0.77)。UVA汇总敏感性、特异性和AUC分别为0.49(95%CI 0.33 - 0.65)、0.91(95%CI 0.84 - 0.96)和0.76(95%CI 0.44 - 0.93)。在汇总分析中观察到显著的异质性。
各个评分的表现从较差到可接受不等。未来的研究应结合不同评分中选定或修改的要素。
部分由英国国家卫生与临床优化研究所(NIHR)资助(17/63/42)。