Appaneal Haley J, Caffrey Aisling R, Lopes Vrishali, Dosa David, LaPlante Kerry L
Infectious Diseases Research Program, Providence Veterans Affairs Medical Center, Providence, RI 02908, USA.
Center of Innovation in Long-Term Support Services, Providence Veterans Affairs Medical Center, Providence, RI 02908, USA.
Antibiotics (Basel). 2023 Jan 20;12(2):224. doi: 10.3390/antibiotics12020224.
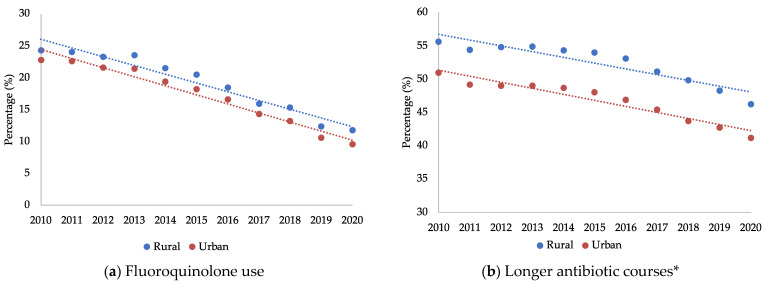
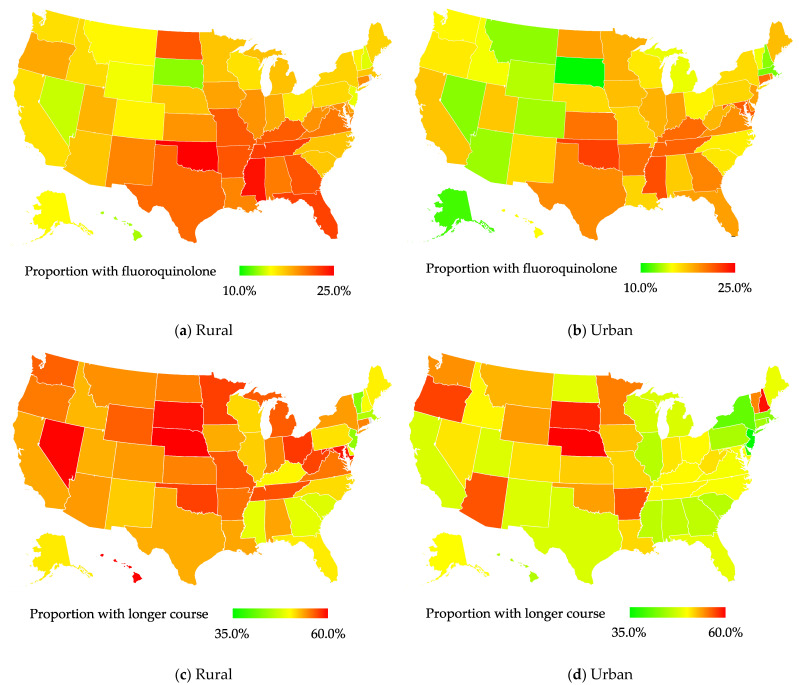
Suboptimal antibiotic prescribing may be more common in patients living in rural versus urban areas due to various factors such as decreased access to care and diagnostic testing equipment. Prior work demonstrated a rural health disparity of overprescribing antibiotics and longer durations of antibiotic therapy in the United States; however, large-scale evaluations are limited. We evaluated the association of rural residence with suboptimal outpatient antibiotic use in the national Veterans Affairs (VA) system. Outpatient antibiotic dispensing was assessed for the veterans diagnosed with an upper respiratory tract infection (URI), pneumonia (PNA), urinary tract infection (UTI), or skin and soft tissue infection (SSTI) in 2010-2020. Rural-urban status was determined using rural-urban commuting area codes. Suboptimal antibiotic use was defined as (1) outpatient fluoroquinolone dispensing and (2) longer antibiotic courses (>ten days). Geographic variation in suboptimal antibiotic use was mapped. Time trends in suboptimal antibiotic use were assessed with Joinpoint regression. While controlling for confounding, the association of rurality and suboptimal antibiotic use was assessed with generalized linear mixed models with a binary distribution and logit link, accounting for clustering by region and year. Of the 1,405,642 veterans diagnosed with a URI, PNA, UTI, or SSTI and dispensed an outpatient antibiotic, 22.8% were rural-residing. In 2010-2020, in the rural- and urban-residing veterans, the proportion of dispensed fluoroquinolones declined by 9.9% and 10.6% per year, respectively. The rural-residing veterans were more likely to be prescribed fluoroquinolones (19.0% vs. 17.5%; adjusted odds ratio (aOR), 1.03; 95% confidence interval (CI), 1.02-1.04) and longer antibiotic courses (53.8% vs. 48.5%; aOR, 1.19, 95% CI, 1.18-1.20) than the urban-residing veterans. Among a large national cohort of veterans diagnosed with URIs, PNA, UTIs, and SSTIs, fluoroquinolone use and longer antibiotic courses were disproportionally more common among rural- as compared to urban-residing veterans. Outpatient antibiotic prescribing must be improved, particularly for rural-residing patients. There are many possible solutions, of which antibiotic stewardship interventions are but one.
由于诸如获得医疗服务和诊断检测设备的机会减少等各种因素,居住在农村地区的患者中,抗生素处方不合理的情况可能比城市地区更为常见。先前的研究表明,在美国,农村地区存在抗生素过度处方和抗生素治疗疗程较长的健康差异;然而,大规模评估有限。我们评估了在国家退伍军人事务(VA)系统中,农村居住情况与门诊抗生素使用不合理之间的关联。对2010年至2020年期间被诊断患有上呼吸道感染(URI)、肺炎(PNA)、尿路感染(UTI)或皮肤及软组织感染(SSTI)的退伍军人的门诊抗生素配药情况进行了评估。使用城乡通勤区号确定城乡状况。抗生素使用不合理的定义为:(1)门诊使用氟喹诺酮类药物;(2)抗生素疗程较长(超过十天)。绘制了抗生素使用不合理情况的地理分布图。使用Joinpoint回归评估抗生素使用不合理情况的时间趋势。在控制混杂因素的同时,使用具有二元分布和logit链接的广义线性混合模型评估农村居住情况与抗生素使用不合理之间的关联,并考虑按地区和年份进行聚类。在1405642名被诊断患有URI、PNA、UTI或SSTI并接受门诊抗生素配药的退伍军人中,22.8%居住在农村。在2010年至2020年期间,农村和城市居住的退伍军人中,每年氟喹诺酮类药物的配药比例分别下降了9.9%和10.6%。与城市居住的退伍军人相比,农村居住的退伍军人更有可能被处方使用氟喹诺酮类药物(19.0%对17.5%;调整后的优势比(aOR)为1.03;95%置信区间(CI)为1.02 - 1.04),且抗生素疗程更长(53.8%对48.5%;aOR为1.19,95%CI为1.18 - 1.20)。在一大群被诊断患有URI、PNA、UTI和SSTI的全国退伍军人队列中,与城市居住的退伍军人相比,农村居住的退伍军人中氟喹诺酮类药物的使用和更长的抗生素疗程比例过高。必须改善门诊抗生素处方,特别是针对农村居住的患者。有许多可能的解决方案,其中抗生素管理干预只是其中之一。