Jurov Iva, Demšar Jure, McCurdy Thomas
Sports Medicine Centre, Clinical Institute of Occupational, Traffic and Sports Medicine, University Medical Centre Ljubljana, 1000 Ljubljana, Slovenia.
Faculty of Computer and Information Science, University of Ljubljana, 1000 Ljubljana, Slovenia.
Life (Basel). 2023 Jan 19;13(2):276. doi: 10.3390/life13020276.
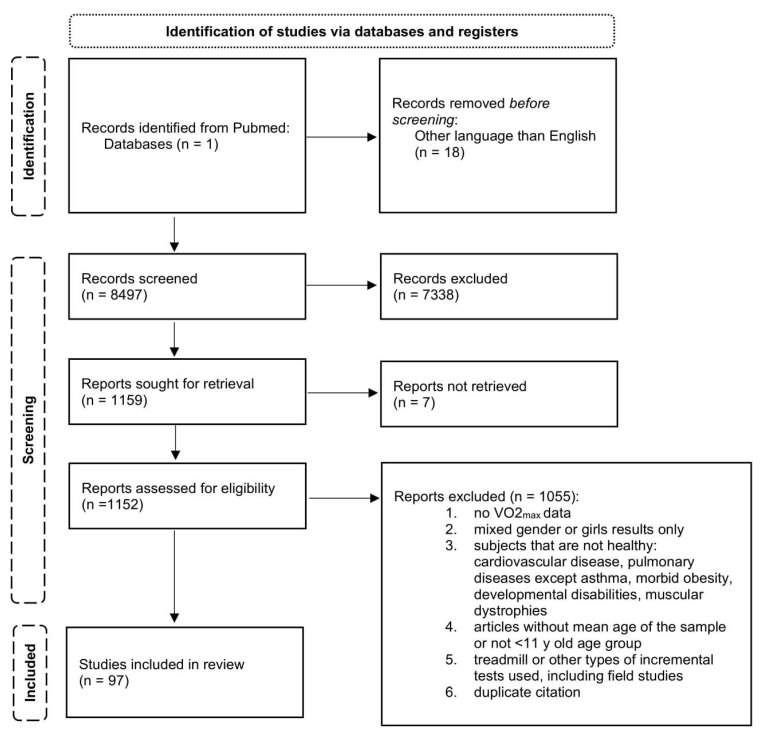
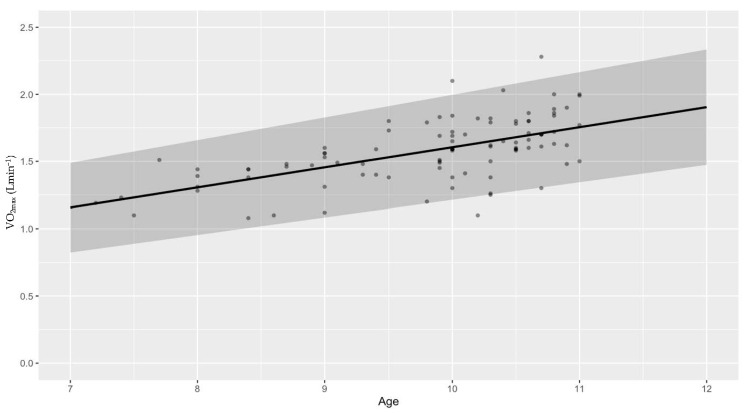
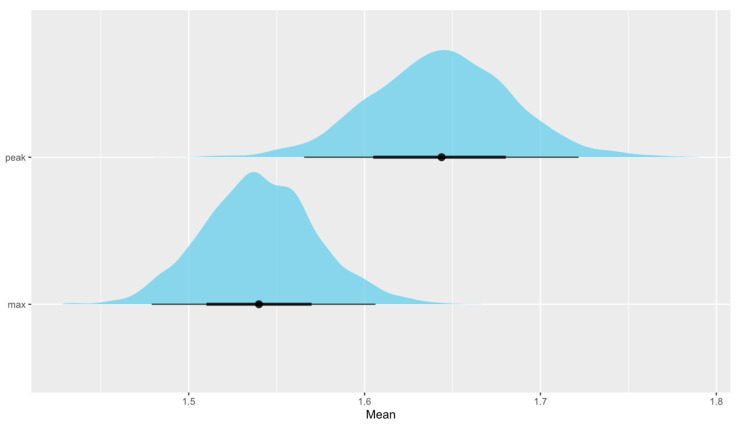
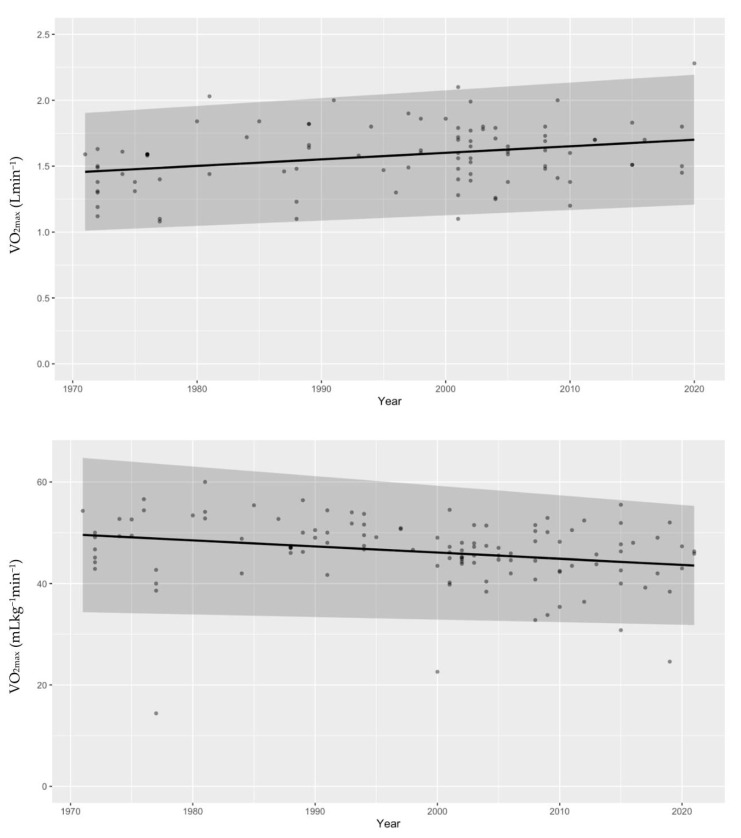
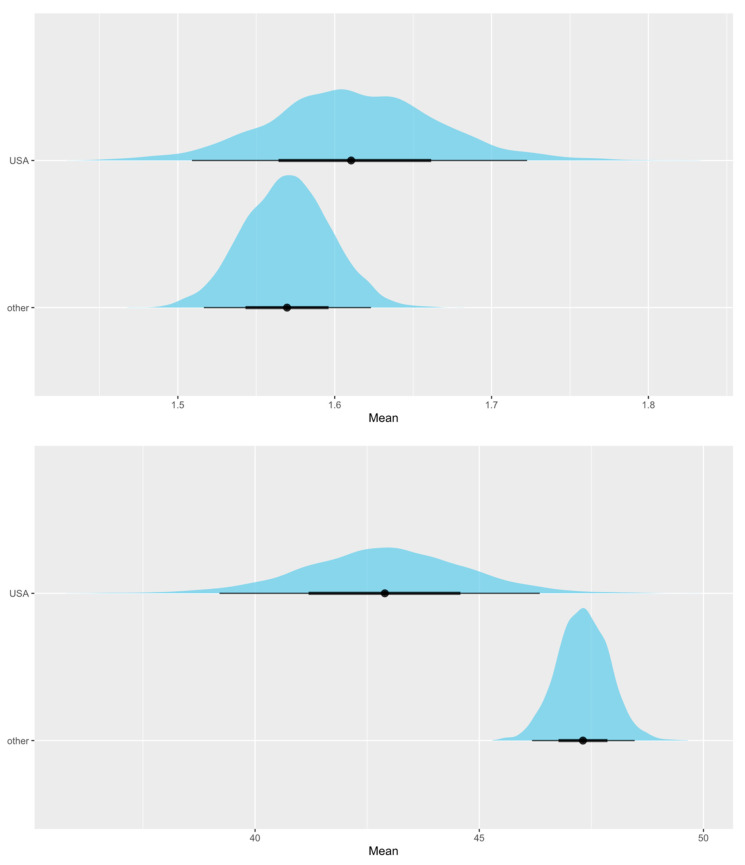
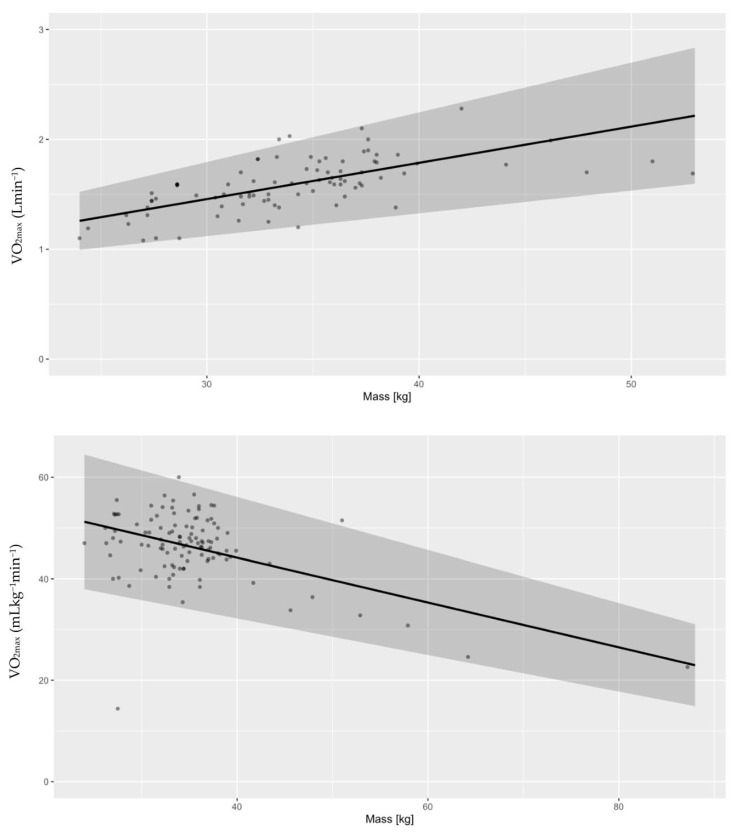
The aim of this study was to develop distributions of VO based on measured values that exist in the literature in prepubertal boys using cycle ergometry. PRISMA guidelines were followed in conducting this research. One database was searched for peak and maximal VO values in healthy boys with mean age under 11 years old. Data were split into articles reporting absolute and relative VO values and analyzed accordingly. Multilevel models grounded in Bayesian principles were used. We investigated associations between VO and body mass, year of the study, and country of origin. Differences in "peak" and "maximal" VO were assessed. Absolute VO (Lmin) increases with age (P ~100%) but mean relative VO does not change (P ~100%). Absolute VO is higher in more recent studies (P = 95.7 ± 0.3%) and mean relative VO is lower (P = 99.6 ± 0.1%). Relative VO in the USA is lower compared with boys from other countries (P = 98.8 ± 0.2%), but there are no differences in absolute values. Mean aerobic capacity estimates presented as "peak" values are higher than "maximal" values on an absolute basis (P = 97.5 ± 0.3%) but not on a relative basis (P = 99.6 ± 0.1%). Heavier boys have lower cardiorespiratory fitness (P ≈ 100%), and body mass seems to be increasing faster with age in the USA compared with other countries (P = 92.3 ± 0.3%). New reference values for cardiorespiratory fitness are presented for prepubertal boys obtained with cycle ergometry. This is new, as no reference values have been determined so far based on actual measured values in prepubertal boys. Aerobic capacity normalized to body weight does not change with age. Cardiorespiratory fitness in prepubertal boys is declining, which is associated with increasing body mass over the last few decades. Lastly, this study did not find any statistically significant difference in the sample's mean aerobic capacity estimates using the "peak" and "maximum" distinctions identified in the literature.
本研究的目的是基于青春期前男孩使用自行车测力计的文献测量值来制定最大摄氧量(VO)分布。本研究遵循PRISMA指南。在一个数据库中搜索了平均年龄在11岁以下的健康男孩的峰值和最大VO值。数据被分为报告绝对和相对VO值的文章并进行相应分析。使用了基于贝叶斯原理的多级模型。我们研究了VO与体重、研究年份和原产国之间的关联。评估了“峰值”和“最大”VO的差异。绝对VO(L/min)随年龄增加(P≈100%),但平均相对VO不变(P≈100%)。在最近的研究中绝对VO更高(P = 95.7±0.3%),平均相对VO更低(P = 99.6±0.1%)。与其他国家的男孩相比,美国男孩的相对VO更低(P = 98.8±0.2%),但绝对值没有差异。以“峰值”表示的平均有氧能力估计值在绝对值上高于“最大”值(P = 97.5±0.3%),但在相对值上并非如此(P = 99.6±0.1%)。体重较重的男孩心肺适能较低(P≈100%),与其他国家相比,美国男孩的体重似乎随年龄增长更快(P = 92.3±0.3%)。给出了青春期前男孩使用自行车测力计获得的心肺适能新参考值。这是新的,因为到目前为止尚未根据青春期前男孩的实际测量值确定参考值。按体重标准化的有氧能力不随年龄变化。青春期前男孩的心肺适能正在下降,这与过去几十年体重增加有关。最后,本研究在使用文献中确定的“峰值”和“最大值”区分的样本平均有氧能力估计值中未发现任何统计学上的显著差异。