Martin-Rincon Marcos, Calbet Jose A L
Department of Physical Education, University of Las Palmas de Gran Canaria, Las Palmas de Gran Canaria, Spain.
Research Institute of Biomedical and Health Sciences (IUIBS), University of Las Palmas de Gran Canaria, Las Palmas de Gran Canaria, Spain.
Front Physiol. 2020 Sep 3;11:1070. doi: 10.3389/fphys.2020.01070. eCollection 2020.
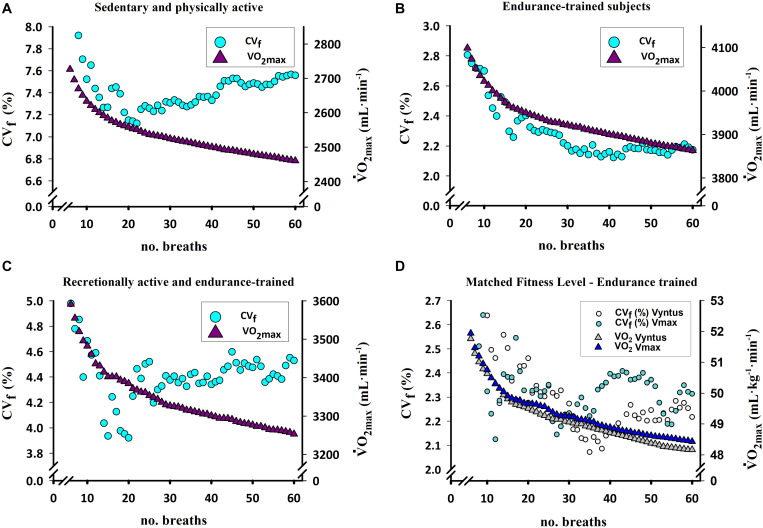
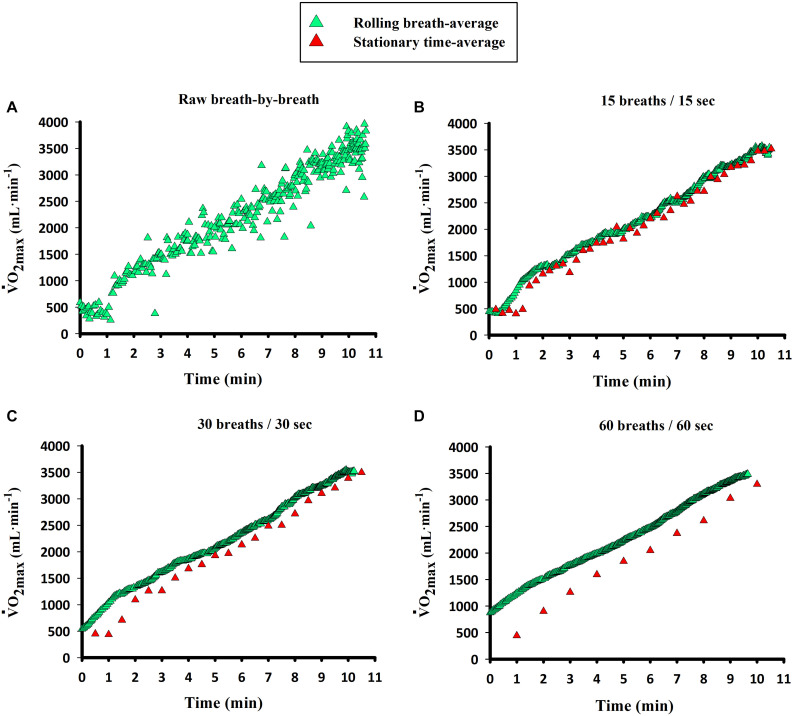
The maximal oxygen uptake ( O) is the primary determinant of endurance performance in heterogeneous populations and has predictive value for clinical outcomes and all-cause mortality. Accurate and precise measurement of O requires the adherence to quality control procedures, including combustion testing and the use of standardized incremental exercise protocols with a verification phase preceded by an adequate familiarization. The data averaging strategy employed to calculate the O from the breath-by-breath data can change the O value by 4-10%. The lower the number of breaths or smaller the number of seconds included in the averaging block, the higher the calculated O value with this effect being more prominent in untrained subjects. Smaller averaging strategies in number of breaths or seconds (less than 30 breaths or seconds) facilitate the identification of the plateau phenomenon without reducing the reliability of the measurements. When employing metabolic carts, averaging intervals including 15-20 breaths or seconds are preferable as a compromise between capturing the true O and identifying the plateau. In training studies, clinical interventions and meta-analysis, reporting of O in absolute values and inclusion of protocols and the averaging strategies arise as imperative to permit adequate comparisons. Newly developed correction equations can be used to normalize O to similar averaging strategies. A lack of improvement of O with training does not mean that the training program has elicited no adaptations, since peak cardiac output and mitochondrial oxidative capacity may be increased without changes in O.
最大摄氧量(VO₂max)是异质人群耐力表现的主要决定因素,对临床结局和全因死亡率具有预测价值。准确精确地测量VO₂max需要遵循质量控制程序,包括燃烧测试以及使用标准化递增运动方案,并在充分熟悉之前有一个验证阶段。用于根据逐次呼吸数据计算VO₂max的数据平均策略可使VO₂max值改变4% - 10%。平均区间内包含的呼吸次数越少或秒数越少,计算出的VO₂max值越高,这种效应在未经训练的受试者中更为突出。在呼吸次数或秒数方面采用较小的平均策略(少于30次呼吸或秒数)有助于识别平台现象,同时又不会降低测量的可靠性。使用代谢车时,15 - 20次呼吸或秒数的平均区间作为捕捉真实VO₂max和识别平台之间的折衷方案较为可取。在训练研究、临床干预和荟萃分析中,以绝对值报告VO₂max并纳入方案和平均策略对于进行充分比较至关重要。新开发的校正方程可用于将VO₂max标准化为类似的平均策略。训练后VO₂max没有提高并不意味着训练计划没有引起适应性变化,因为即使VO₂max没有变化,峰值心输出量和线粒体氧化能力也可能增加。