Miselli Francesca, Crestani Sara, Maugeri Melissa, Passini Erica, Spaggiari Valentina, Deonette Elisa, Ćosić Branislava, Rossi Katia, Roversi Maria Federica, Bedetti Luca, Lugli Licia, Costantini Riccardo Cuoghi, Berardi Alberto
PhD Program in Clinical and Experimental Medicine, University of Modena and Reggio Emilia, 41121 Modena, Italy.
Neonatal Intensive Care Unit, University Hospital of Modena, 41124 Modena, Italy.
Microorganisms. 2023 Feb 3;11(2):396. doi: 10.3390/microorganisms11020396.
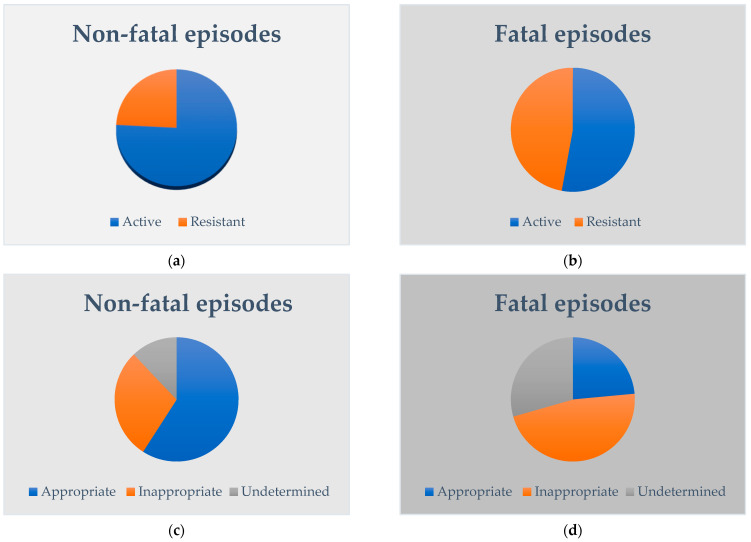
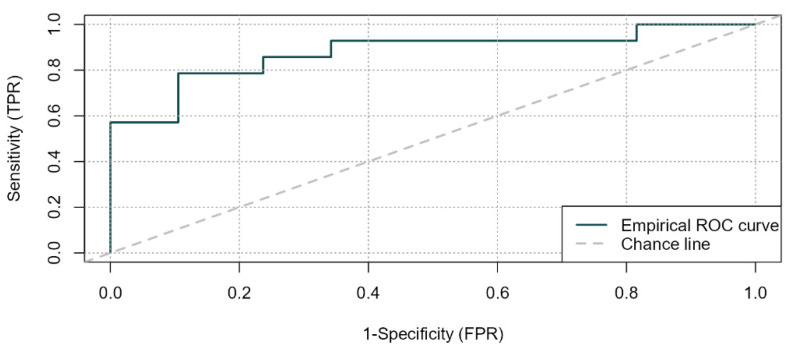
To investigate the impact of timing, in vitro activity and appropriateness of empirical antimicrobials on the outcome of late-onset sepsis among preterm very low birth weight infants that are at high risk of developing meningitis. This retrospective study included 83 LOS episodes in 73 very low birth weight infants born at ≤32 weeks' gestation with positive blood and/or cerebrospinal fluid culture or polymerase chain reaction at >72 h of age. To define the appropriateness of empirical antimicrobials we considered both their in vitro activity and their ideal delivery through the blood-brain barrier when meningitis was confirmed or not ruled out through a lumbar puncture. The primary outcome was sepsis-related mortality. The secondary outcome was the development of brain lesions. Timing, in vitro activity and appropriateness of empirical antimicrobials, were compared between fatal and non-fatal episodes. Uni- and multi-variable analyses were carried out for the primary outcome. Time to antibiotics and in vitro activity of empirical antimicrobials were similar between fatal and non-fatal cases. By contrast, empirical antimicrobials were appropriate in a lower proportion of fatal episodes of late-onset sepsis (4/17, 24%) compared to non-fatal episodes (39/66, 59%). After adjusting for Gram-negative vs. Gram-positive pathogen and for other supportive measures (time to volume administration), inappropriate empirical antimicrobials remained associated with mortality (aOR, 10.3; 95% CI, 1.4-76.8, = 0.023), while timing to first antibiotics was not (aOR 0.9; 95% CI, 0.7-1.2, = 0.408; AUC = 0.88). The association between appropriate antimicrobials and brain sequelae was also significant ( = 0.024). The risk of sepsis-related mortality and brain sequelae in preterm very low birth weight infants is significantly associated with the appropriateness (rather than the timing and the in vitro activity) of empirical antimicrobials. Until meningitis is ruled out through lumbar puncture, septic very low birth weight infants at high risk of mortality should receive empiric antimicrobials with high delivery through the blood-brain barrier.
为研究经验性抗菌药物的用药时机、体外活性及合理性对极早产极低出生体重且有发生脑膜炎高风险婴儿迟发性败血症结局的影响。这项回顾性研究纳入了73例孕周≤32周的极低出生体重婴儿中的83次迟发性败血症发作,这些婴儿在出生72小时后血培养和/或脑脊液培养或聚合酶链反应呈阳性。为界定经验性抗菌药物的合理性,我们既考虑了其体外活性,也考虑了在通过腰椎穿刺确诊或未排除脑膜炎时其透过血脑屏障的理想给药情况。主要结局是败血症相关死亡率。次要结局是脑损伤的发生。比较了致命性和非致命性发作之间经验性抗菌药物的用药时机、体外活性及合理性。对主要结局进行了单变量和多变量分析。致命性和非致命性病例之间抗生素给药时间和经验性抗菌药物的体外活性相似。相比之下,迟发性败血症致命性发作中经验性抗菌药物合理的比例(4/17,24%)低于非致命性发作(39/66,59%)。在对革兰氏阴性菌与革兰氏阳性菌病原体以及其他支持性措施(液体输注时间)进行校正后,经验性抗菌药物不合理仍与死亡率相关(校正后比值比,10.3;95%置信区间,1.4 - 76.8,P = 0.023),而首次使用抗生素的时间则不然(校正后比值比0.9;95%置信区间,