The George Institute for Global Health, UNSW, Sydney, Australia.
Department of Clinical Sciences, Center for Primary Health Care Research, Lund University, Malmö, Sweden.
Glob Heart. 2023 Feb 23;18(1):7. doi: 10.5334/gh.1184. eCollection 2023.
To assess whether inter-professional, bidirectional collaboration between general practitioners (GPs) and pharmacists has an impact on improving cardiovascular risk outcomes among patients in the primary care setting. It also aimed to understand the different types of collaborative care models used.
Systematic review and Hartung-Knapp-Sidik-Jonkman random effects meta-analyses of randomised control trials (RCTs) in inter-professional bidirectional collaboration between GP and pharmacists assessing a change of patient cardiovascular risk in the primary care setting.
MEDLINE, EMBASE, Cochrane, CINAHL and International Pharmaceutical Abstracts, scanned reference lists of relevant studies, hand searched key journals and key papers until August 2021.
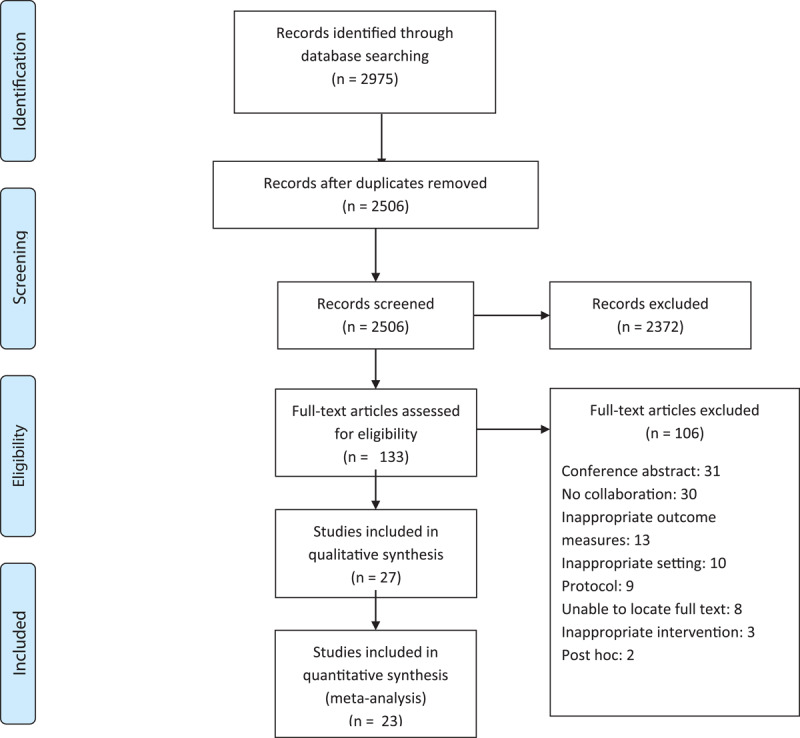
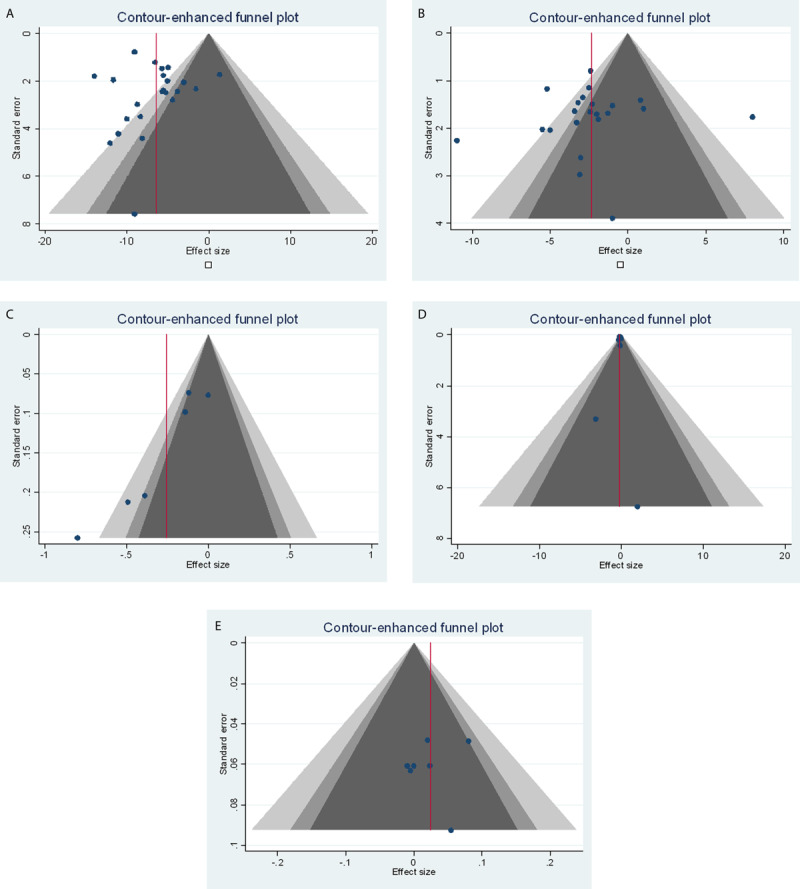
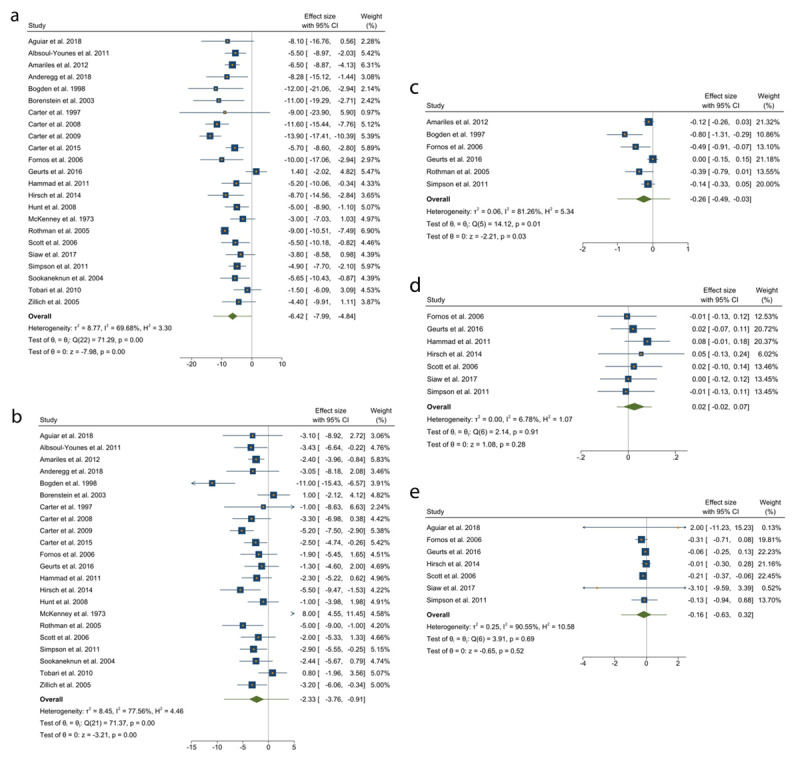
Twenty-eight RCTs were identified. Collaboration was associated with significant reductions in systolic and diastolic blood pressure (23 studies, 5,620 participants) of -6.42 mmHg (95% confidence interval (95%CI) -7.99 to -4.84) and -2.33 mmHg (95%CI -3.76 to -0.91), respectively. Changes in other cardiovascular risk factors included total cholesterol (6 studies, 1,917 participants) -0.26 mmol/L (95%CI -0.49 to -0.03); low-density lipoprotein (8 studies, 1,817 participants) -0.16 mmol/L (95%CI -0.63 to 0.32); high-density lipoprotein (7 studies, 1,525 participants) 0.02 mmol/L (95%CI -0.02 to 0.07). Reduction in haemoglobin A1c (HbA1C) (10 studies, 2,025 participants), body mass index (8 studies, 1,708 participants) and smoking cessation (1 study, 132 participants) was observed with GP-pharmacist collaboration. Meta-analysis was not conducted for these changes. Various models of collaborative care included verbal communication (via phone calls or face to face), and written communication (emails, letters). We found that co-location was associated with positive changes in cardiovascular risk factors.
Although it is clear that collaborative care is ideal compared to usual care, greater details in the description of the collaborative model of care in studies is required for a core comprehensive evaluation of the different models of collaboration.
评估全科医生(GP)和药剂师之间的专业间、双向协作是否会影响改善初级保健环境中患者的心血管风险结果。它还旨在了解使用的不同类型的协作护理模式。
对 GP 和药剂师之间专业间双向协作的随机对照试验(RCT)进行系统评价和 Hartung-Knapp-Sidik-Jonkman 随机效应荟萃分析,评估初级保健环境中患者心血管风险的变化。
MEDLINE、EMBASE、Cochrane、CINAHL 和国际药学文摘,扫描相关研究的参考文献列表,手检关键期刊和关键论文,直到 2021 年 8 月。
确定了 28 项 RCT。协作与收缩压和舒张压的显著降低相关(23 项研究,5620 名参与者)分别为-6.42mmHg(95%置信区间(95%CI)-7.99 至-4.84)和-2.33mmHg(95%CI-3.76 至-0.91)。其他心血管风险因素的变化包括总胆固醇(6 项研究,1917 名参与者)-0.26mmol/L(95%CI-0.49 至-0.03);低密度脂蛋白(8 项研究,1817 名参与者)-0.16mmol/L(95%CI-0.63 至 0.32);高密度脂蛋白(7 项研究,1525 名参与者)0.02mmol/L(95%CI-0.02 至 0.07)。观察到 GP-药剂师协作与血红蛋白 A1c(HbA1C)降低(10 项研究,2025 名参与者)、体重指数(8 项研究,1708 名参与者)和戒烟(1 项研究,132 名参与者)有关。对于这些变化,未进行荟萃分析。协作护理的各种模式包括口头交流(通过电话或面对面)和书面交流(电子邮件、信件)。我们发现,共同定位与心血管风险因素的积极变化有关。
虽然协作护理明显优于常规护理,但需要在研究中更详细地描述协作护理模式,以便对不同的协作模式进行全面评估。